Why does my jaw keep locking is one of the most searched health questions in 2026, and for good reason — a jaw that repeatedly locks open or shut is not just uncomfortable, it is a signal that something is wrong with one of the most used joints in your body.
The temporomandibular joint moves every time you speak, chew, yawn, or swallow.
When it starts locking regularly, the underlying cause needs attention before the damage becomes permanent.
The temporomandibular joint, commonly called the TMJ, connects your lower jawbone to your skull on each side of your face. You can feel both joints by placing your fingertips just in front of your ears and opening your mouth slowly.
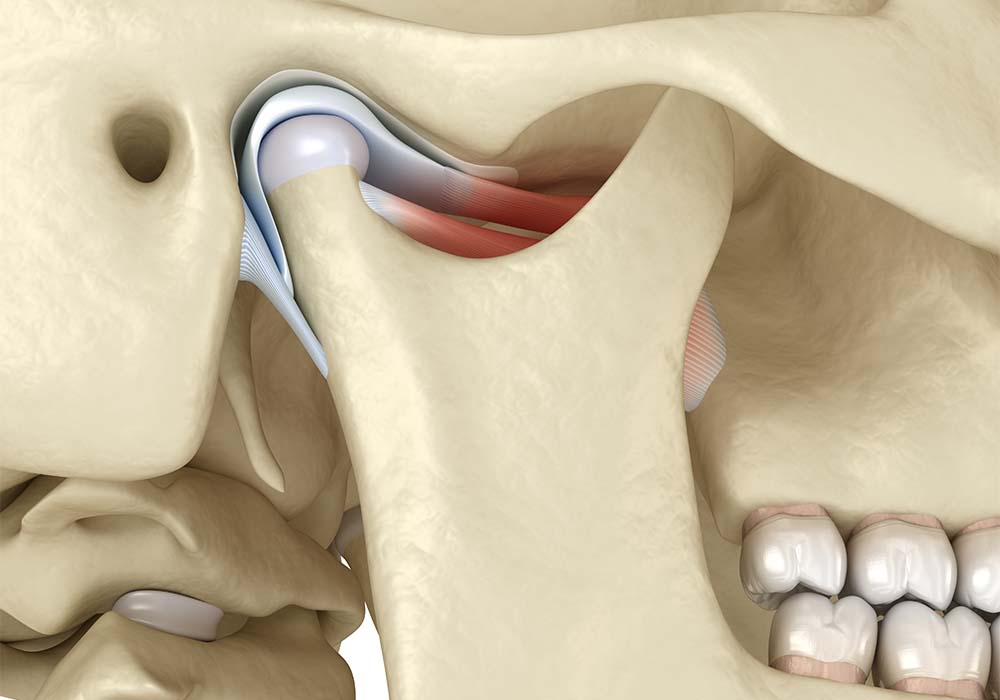
Inside each joint is a small cartilage disc that acts as a cushion, allowing the joint to glide smoothly during movement. When this disc shifts out of position, wears down, or becomes inflamed, the joint cannot move correctly — and locking is one of the most common results.
TMJ disorders, also referred to as TMD (temporomandibular disorders), affect an estimated 5 to 12 percent of the general adult population. Women between the ages of 20 and 60 are disproportionately affected, though the condition can occur at any age and in any gender.
There are two distinct types of jaw locking, and understanding the difference matters for how you respond.
Closed locking happens when the jaw is stuck in a partially or fully closed position and cannot open properly. This is the more common form and is usually associated with TMJ disc displacement.
Open locking happens when the jaw is stuck open and cannot close. This is less common but often more alarming. It frequently occurs after a wide yawn, prolonged dental treatment, or a sudden movement. Open locking typically requires professional manipulation to resolve and should be treated as an urgent situation.
| Type of Locking | Position | Common Cause | Urgency |
|---|---|---|---|
| Closed Locking | Jaw stuck shut or barely open | Disc displacement, muscle spasm | See dentist or doctor promptly |
| Open Locking | Jaw stuck open | Joint dislocation, trauma | Urgent — seek care immediately |
| Intermittent Locking | Locks and releases repeatedly | Early TMJ disc displacement | Schedule evaluation |
| Progressive Locking | Worsening over time | Arthritis, advanced disc damage | Do not delay treatment |
The single most common cause of a jaw that keeps locking is displacement of the cartilage disc inside the temporomandibular joint. When this disc shifts forward or to the side, it blocks the normal gliding motion of the joint.
In the early stages, you will often notice a clicking or popping sound when you open or close your mouth. This is the disc snapping back into position temporarily. Over time, the disc may stop relocating, leading to the locking that many patients describe as sudden, frightening, and painful.
Without treatment, the disc can deteriorate to the point where there is direct bone-to-bone contact inside the joint. At that stage, every jaw movement causes pain and the condition becomes significantly harder to manage.
Bruxism is the involuntary grinding or clenching of teeth, and it is one of the most significant contributors to repeated jaw locking. The problem with bruxism is that it most commonly occurs during sleep, meaning many people have no idea they are doing it until symptoms appear.
Repeated grinding puts enormous pressure on the TMJ and the surrounding muscles. Over time, this leads to joint strain, cartilage wear, muscle fatigue, and eventually the disc displacement that causes locking.
Signs that bruxism may be causing your jaw locking include waking up with jaw soreness or headaches, a partner reporting grinding sounds during the night, teeth that appear flattened or worn, and increased tooth sensitivity with no obvious dental cause.

Chronic stress is a major and often underappreciated driver of jaw locking. Stress causes people to unconsciously clench their jaw muscles — both during the day and at night — creating sustained tension that overloads the TMJ.
Muscle tension from stress can also cause the jaw to lock without any underlying disc displacement. The muscles responsible for closing the jaw go into a prolonged contraction, which physically limits how far the mouth can open.
Managing stress is not just good advice — it is a legitimate medical intervention when jaw locking is caused by stress-related muscle tension. Deep breathing, mindfulness, yoga, and progressive muscle relaxation have all shown measurable benefit in reducing TMJ symptoms.
Both rheumatoid arthritis and osteoarthritis can affect the temporomandibular joint directly. Rheumatoid arthritis is an autoimmune condition that causes joint inflammation, while osteoarthritis involves the gradual wearing down of joint cartilage over time.
In both cases, the protective cartilage inside the TMJ is damaged. The joint surface becomes rough and uneven, and the disc may be affected as well. This leads to a jaw that clicks, grinds, and eventually locks as the normal mechanics of the joint break down.
Jaw locking caused by arthritis tends to be progressive. It typically gets worse over time without treatment and may be accompanied by morning stiffness, general joint pain elsewhere in the body, and visible swelling around the jaw area.
A blow to the face, a sports injury, an accident, or even a fall can damage the structures inside or around the TMJ. The cartilage disc can be knocked out of position, the surrounding ligaments can be torn, and the joint capsule can be damaged — all of which can lead to immediate or delayed jaw locking.
Blunt force trauma to the jaw does not always cause immediate symptoms. In some cases, the initial injury heals without treatment, but scar tissue and ligament changes cause locking to develop weeks or even months later.
If you have had any significant jaw injury in your history and are now experiencing locking, the two events are almost certainly connected.
Extended dental procedures that require keeping the mouth wide open for long periods can strain the TMJ and trigger locking. Root canals, wisdom tooth extractions, and implant placements are among the procedures most frequently cited by patients who develop jaw locking afterward.
The trigeminal nerve, which controls facial muscle movement, can also be irritated during local anesthetic injections. Irritation of this nerve can contribute to muscle tension and locking in the days following a dental visit.
If you regularly experience jaw locking after dental appointments, inform your dentist. Many practices can use bite blocks or schedule shorter appointments to reduce the strain on your TMJ during treatment.
Wisdom teeth that erupt in a poor position or become impacted can contribute to jaw locking in multiple ways. Infected wisdom teeth cause swelling in the surrounding tissues that physically restricts jaw movement.
Poorly positioned wisdom teeth can also push against the adjacent structures of the jaw, altering the mechanics of how the joint moves. In these cases, extraction of the problematic wisdom teeth often resolves or significantly reduces the locking.
If your jaw locking developed around the same time your wisdom teeth began erupting, this connection is worth discussing with an oral surgeon.
A tooth abscess or any significant oral infection near the jaw can cause swelling and muscle spasm that leads to locking. The infection itself inflames the surrounding tissue, and the body’s protective response restricts jaw movement to prevent further damage.
While this form of jaw locking usually resolves once the infection is treated, untreated infections can permanently damage the muscles or nerves in the area, leading to repeated bouts of locking that persist long after the infection is gone.
Any jaw locking that is accompanied by fever, significant swelling, a bad taste in the mouth, or tooth pain should be evaluated immediately, as it may indicate an active infection requiring urgent dental care.
Tetanus, also called lockjaw, is a bacterial infection caused by Clostridium tetani that causes painful muscle contractions throughout the body, starting with the jaw and neck. This is a medical emergency and is entirely different from TMJ-related locking.
Tetanus-related jaw locking is typically accompanied by muscle stiffness spreading to other areas, difficulty swallowing, fever, and muscle spasms that worsen with stimulation. This combination of symptoms distinguishes it clearly from TMJ locking, which does not cause systemic muscle involvement.
If you have not been vaccinated against tetanus and experience jaw locking with any of the systemic symptoms described above, go to an emergency room immediately.
Most cases of jaw locking, while painful and alarming, are not medical emergencies. However, several situations require immediate medical attention.
Seek urgent care if your jaw locks completely open and cannot close even slightly. This type of open dislocation can cause tissue and nerve damage if left untreated for too long.
Go to an emergency room if jaw locking is accompanied by fever, visible and worsening swelling, difficulty breathing or swallowing, significant pain spreading to your neck and chest, or numbness in your face. These combinations suggest infection, abscess, or a neurological issue that needs urgent evaluation.
Jaw locking that gets progressively worse over weeks or months should be evaluated promptly by a dentist or TMJ specialist. If the frequency or severity of locking is increasing, the underlying damage is likely advancing.
Other progressive warning signs include an increasing inability to open your mouth fully, changes in how your teeth fit together when you bite down, visible facial asymmetry developing over time, and persistent ear pain or the sensation of fullness in one or both ears.
Delaying treatment for progressive TMJ issues significantly increases the complexity and cost of treatment. What can often be managed conservatively in early stages may eventually require surgical intervention if ignored.
| Symptom | Likely Cause | Action Needed |
|---|---|---|
| Jaw locks and releases with a click | Disc displacement — early stage | See dentist, consider night guard |
| Jaw locks fully closed, very painful | Advanced disc displacement or muscle spasm | Dentist or oral surgeon promptly |
| Jaw locks open after yawning | Joint dislocation | Urgent — seek care same day |
| Locking with fever and swelling | Infection or abscess | Emergency care immediately |
| Locking with neck stiffness and muscle spasms | Possible tetanus | Emergency room immediately |
| Morning jaw stiffness with clicking | Bruxism and/or early TMJ disorder | Dental evaluation and night guard |
| Locking after dental procedure | TMJ strain from prolonged opening | Contact your dentist |
| Worsening locking over months | Progressive arthritis or disc deterioration | TMJ specialist evaluation |

A dentist or doctor evaluating jaw locking will start with a thorough history of your symptoms — when the locking started, how often it occurs, what triggers it, and what makes it better or worse.
A physical examination will check for tenderness in the jaw muscles, listen for clicking or grinding sounds during movement, and measure how far you can open your mouth. Normal mouth opening is typically around 40 to 50 millimeters — approximately three fingers’ width. Significantly less than this suggests restricted joint movement.
Imaging is frequently needed to understand what is happening inside the joint. X-rays can show bone changes and joint space narrowing. CT scans provide detailed bone structure images. MRI is the gold standard for visualizing the soft tissue disc and identifying displacement or damage.
TMJ disorders are frequently misdiagnosed because their symptoms overlap with several other conditions. Ear pain from TMJ locking is commonly mistaken for an ear infection. Jaw pain can mimic toothache. Headaches related to jaw tension are often treated as tension headaches or migraines without the underlying TMJ cause being addressed.
Trigeminal neuralgia, which affects the same nerve that serves the TMJ, can produce facial pain easily confused with jaw joint problems. Swollen lymph nodes, salivary gland disease, and even giant cell arteritis have all been documented as conditions initially confused with TMJ disorders.
If you have been treated repeatedly for ear infections, toothaches, or headaches without resolution, consider asking your doctor specifically about TMJ evaluation.
Applying heat to the jaw muscles helps relax muscle tension that is contributing to locking. Use a warm, damp towel or a heat pack for 10 to 15 minutes at a time. Heat works best for muscle-related stiffness and tension.
Cold therapy is more effective for acute pain and swelling. An ice pack wrapped in a cloth applied for 10 minutes can reduce inflammation and numb sharp pain after a locking episode. Alternating heat and cold can be helpful when both inflammation and muscle tension are present.
Gentle jaw exercises can improve mobility, reduce stiffness, and strengthen the supporting muscles around the TMJ. These exercises should never cause sharp pain — work within a comfortable range only.
The goldfish exercise is one of the most recommended. Rest your tongue on the roof of your mouth just behind your upper front teeth. With one finger on your chin and one on your TMJ, gently drop your lower jaw halfway, then close. Repeat six times, completing one full set. Do this six times per day.
The chin tuck exercise helps improve posture, which has a direct effect on jaw tension. Drop your chin straight down toward your chest, hold for three seconds, and return. Poor forward head posture significantly increases the strain placed on the TMJ.
Resisted mouth opening is a strengthening exercise. Place your thumb under your chin, gently push upward for mild resistance, then slowly open your mouth against that resistance. Hold three to six seconds, then close slowly. This builds the muscles that support jaw opening.
A soft diet dramatically reduces the mechanical load on the TMJ during periods of locking or increased pain. Avoid hard, chewy, or crunchy foods — anything that requires significant chewing force or wide jaw opening.
Foods to avoid during a flare include raw carrots, hard bread, nuts, tough meat, gum, and ice. Foods that work well include scrambled eggs, yogurt, mashed potatoes, smoothies, soft fish, and soups.
Even after the acute phase passes, maintaining a diet that limits extreme chewing stress helps prevent repeat flare-ups.
Breaking certain habits significantly reduces the daily stress placed on the TMJ. Stop chewing gum — it keeps the jaw muscles in constant contraction and accelerates joint wear. Stop biting your nails, pencils, or any non-food object, as these habits create repetitive jaw strain.
Avoid resting your chin or jaw in your hand, as this applies external pressure to the joint. During yawning, support your lower jaw gently with your hand to prevent the wide opening that can trigger locking.
Improve your posture, particularly if you work at a desk. Forward head posture increases tension in the neck and jaw muscles significantly. A properly adjusted workstation and regular posture breaks can make a measurable difference in jaw symptoms.
A dental night guard is one of the most widely recommended treatments for TMJ locking related to bruxism and disc displacement. Night guards are custom-fitted oral devices worn during sleep that prevent teeth grinding and slightly reposition the jaw to reduce joint pressure.
Over-the-counter night guards are available but are generally less effective than custom-fitted devices made by a dentist. Custom guards allow for adjustable thickness based on the specific severity and nature of your TMJ condition.
Occlusal splints are similar devices that can be worn during the day as well as at night, and they are often used to actively reposition the jaw over time rather than simply protect it during grinding.
A physical therapist trained in TMJ disorders can provide targeted treatment that goes beyond what home exercises alone can achieve. This includes manual therapy techniques to improve joint mobility, dry needling for muscle trigger points, ultrasound therapy to reduce deep tissue inflammation, and postural correction work that addresses neck and shoulder tension contributing to jaw problems.
Physical therapy is particularly effective when jaw locking is primarily driven by muscle dysfunction rather than structural disc damage. It is often recommended as a first-line treatment before more invasive options are considered.
Over-the-counter NSAIDs such as ibuprofen or naproxen can reduce inflammation and pain during acute locking episodes. These should be used short-term and as directed.
For more persistent muscle tension, a doctor may prescribe short-term muscle relaxants. These are typically not a long-term solution but can help break cycles of severe muscle spasm.
Corticosteroid injections directly into the TMJ reduce inflammation effectively in cases where joint inflammation is a primary driver. These injections are generally used when conservative measures have not produced sufficient relief.
Antidepressants at low doses are sometimes prescribed for chronic TMJ pain, as they have been shown to have pain-modulating effects independent of their antidepressant function.
Surgery is the last resort for jaw locking and is reserved for cases where conservative treatment has failed to produce acceptable results. The least invasive surgical option is arthrocentesis, which involves flushing the joint with sterile fluid to remove inflammatory byproducts and restore disc mobility.
Arthroscopy uses a tiny camera inserted into the joint to identify and address specific structural problems while minimizing recovery time.
Open joint surgery is the most invasive option and is reserved for severe structural damage, including significantly displaced or deteriorated discs and cases of advanced arthritis where joint reconstruction is necessary.
Preventing repeat locking requires consistent attention to the habits and factors that stress the TMJ. Wear a night guard if you grind your teeth — this is one of the most impactful protective measures available and significantly reduces the long-term risk of disc damage.
Manage stress actively. Stress-driven jaw clenching is one of the leading contributors to TMJ disorders, and no other treatment will hold long-term if stress is continuously triggering muscle tension in the jaw.
Maintain good posture throughout your workday. Use an ergonomic chair and monitor height that prevents forward head posture. Take posture breaks every 30 minutes if you work at a desk.
Eat a diet rich in calcium and magnesium, which support healthy muscle function and joint cartilage. Avoid habits that place unnecessary stress on the joint — no gum, no nail biting, no ice chewing.
Schedule regular dental check-ups. A dentist can identify early signs of TMJ stress — worn tooth surfaces, bite changes, early disc displacement sounds — before they progress to the point of causing locking.
Painless locking usually means the disc is displacing and returning without causing inflammation yet — but it is still an early warning sign that the joint mechanics are compromised and need evaluation.
Yes. Stress-driven muscle clenching can create enough tension to physically restrict jaw movement without any disc displacement or structural damage being present at all.
Open locking where the jaw cannot close is urgent and needs same-day care. Intermittent closed locking is not an emergency but does require prompt evaluation to prevent progression.
A TMJ-related locking episode can last anywhere from a few minutes to several days. Frequent or prolonged episodes are a clear sign that professional treatment is overdue.
Some mild, early-stage cases do resolve with rest and home care. However, repeated locking without treatment typically worsens over time as the underlying disc and joint damage progresses.
Apply gentle warm heat to the jaw muscles, massage the masseter muscle in circular motions with medium finger pressure, and try slow, gentle side-to-side jaw movements. Do not force the jaw open.
A properly fitted night guard reduces grinding and repositions the jaw to lower stress on the disc. It significantly reduces the frequency of locking in bruxism-related cases but may not eliminate locking caused by advanced disc displacement.
Yes. Forward head posture increases tension in the neck and jaw muscles significantly. Poor posture is a contributing factor in many TMJ cases and correcting it is part of effective treatment.
Start with your dentist, who can perform an initial TMJ evaluation. You may be referred to an oral and maxillofacial surgeon, an orofacial pain specialist, or a physical therapist depending on the cause and severity.
Surgery is rarely the first choice. The majority of jaw locking cases respond well to night guards, physical therapy, medication, and lifestyle changes. Surgery is considered only when conservative measures have been fully explored and have not provided adequate relief.
Why does my jaw keep locking is a question that deserves a clear, direct answer — and that answer is almost always rooted in the temporomandibular joint.
Whether the cause is disc displacement, bruxism, stress, arthritis, injury, or infection, the jaw does not lock repeatedly without a reason.
The warning signs covered in this guide exist to help you recognize when your situation is manageable at home and when it demands professional care.
Most cases of jaw locking respond well to conservative treatment when addressed early — night guards, physical therapy, dietary changes, and stress management are effective tools.
What becomes dangerous is delay. A jaw that locks intermittently today can progress to a joint that causes daily pain and requires surgical intervention if the underlying cause goes untreated.
Take your jaw symptoms seriously in 2026 — seek evaluation, understand your cause, and commit to the treatment that matches your specific situation.