
Why is my pinky toe sideways is a question more people ask than you might expect. The little toe, also called the fifth toe, is the most vulnerable digit on the foot.
It sits exposed on the outer edge, absorbs pressure from shoes, and is often the first toe to shift out of alignment over time. For some people the change happens gradually.
For others, it seems to appear suddenly. Either way, a sideways pinky toe is rarely just a cosmetic issue — it can signal underlying structural changes that deserve attention.
A sideways pinky toe refers to a position where the fifth toe rotates, tilts, or shifts out of its normal alignment. It may angle inward toward the fourth toe, turn outward away from the foot, or curl and tuck slightly underneath the neighboring toe.
The condition can range from mild — just a slight lean — to more pronounced, where the toe fully overlaps or underlaps the adjacent digit. Some people feel no pain at all. Others experience constant irritation, pressure sores, or difficulty walking comfortably in shoes.
The clinical term most commonly used for this condition is adductovarus deformity of the fifth toe, which describes a toe that has rotated inward and downward from its natural position.
Understanding why this happens starts with knowing the structure involved. Your pinky toe is connected to your foot through the fifth metatarsophalangeal (MTP) joint — the knuckle at the base of the little toe. A network of tendons and ligaments holds the toe in place and controls its movement.
When those tendons become weak, tight, or imbalanced — from any cause — the fifth toe begins to drift out of its normal position. Once the shift starts, the ongoing pressure of walking and footwear makes it worse over time. Left untreated, the joint can eventually stiffen in the rotated posture, making correction much harder.
Not all crooked pinky toes look the same. Recognizing which type you have helps narrow down the cause and the best treatment path.
| Type | Description | Common Cause |
|---|---|---|
| Adductovarus Toe | Toe rotates inward and curls downward | Tendon imbalance, tight footwear |
| Overlapping Toe | Fifth toe crosses over the fourth toe | Congenital, bunions, hammertoe |
| Underlapping Toe | Fifth toe slides underneath the fourth toe | Genetic, tendon tightness |
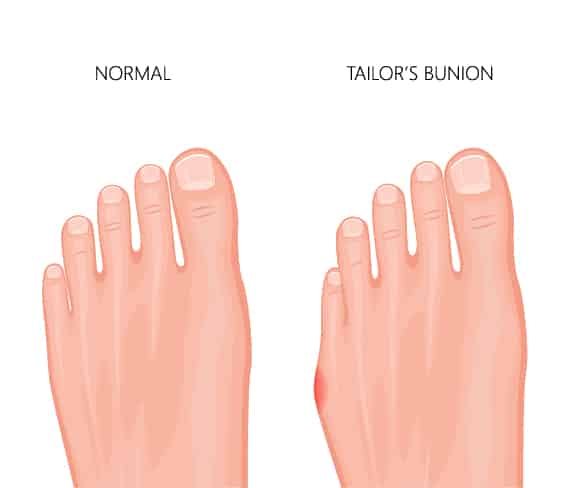
| Tailor’s Bunion (Bunionette) | Bony bump at base forces toe inward | Inherited foot structure, narrow shoes |
Each type can progress from flexible and correctable to rigid and fixed if not addressed early enough.
The single most common contributing factor is shoe choice. Shoes with a narrow or pointed toe box gradually crowd the toes, forcing the pinky toe to rotate or angle inward under constant pressure.
High heels make the problem significantly worse. They shift body weight forward onto the forefoot, compressing all five toes toward the pointed front of the shoe for hours at a time. Over months and years, this repeated mechanical pressure reshapes how the toe sits.
Women are statistically more affected than men for this reason. Even after switching to better footwear, the damage accumulated over years of tight shoes does not automatically reverse.
Genetics plays a major role in who develops a sideways pinky toe. If a parent or sibling has overlapping, underlapping, or rotated toes, the chances of developing the same issue are significantly higher.
Inherited structural factors include the shape of the fifth metatarsal bone, the natural flexibility of the toe joints, and the overall mechanical structure of the foot. Some people are simply born with a predisposition to toe drift.
Approximately 20 to 30 percent of people born with a turned fifth toe have it on both feet, which further points to a genetic origin rather than a purely environmental one.
The tendons that stabilize the little toe must be balanced on all sides to keep the toe pointing straight. When one tendon becomes weaker or tighter than the others — through inactivity, overuse, or injury — the toe is pulled out of alignment.
This imbalance can develop gradually from years of unsupportive footwear, sedentary habits, or changes in gait. Prior injuries or repetitive strain accelerate the process. Even without any single traumatic event, the toe can slowly rotate into the adductovarus posture over time.
Hammertoe is a deformity where one or more toes bend abnormally at the middle joint, creating a claw or hammer shape. When this affects the fifth toe, the abnormal bend often comes with a sideways rotation as well.
Hammertoe in the little toe is commonly caused by muscle imbalance, tight tendons, ill-fitting shoes, and in some cases neurological conditions. It tends to be flexible early on — meaning the toe can still be straightened manually — but becomes rigid and fixed without treatment.
| Feature | Flexible Hammertoe | Rigid Hammertoe |
|---|---|---|
| Can be straightened manually | Yes | No |
| Stage | Early | Advanced |
| Conservative treatment effective | Often yes | Rarely |
| Surgery required | Sometimes | Usually |
A tailor’s bunion, also called a bunionette, is a bony bump that develops at the base of the fifth metatarsophalangeal joint — the outside edge of the foot near the pinky toe. As the metatarsal bone bows outward, the pinky toe is pushed inward, causing it to angle toward the fourth toe.
The condition gets its name from centuries-old tailors who sat cross-legged all day with the outer edge of their feet pressed against hard floors. Today it is caused primarily by an inherited poor or weak mechanical structure of the foot, aggravated by narrow shoes and high heels.
Symptoms include redness, swelling, and pain near the base of the little toe, especially when wearing tight shoes. A callus or corn may develop directly over the bony bump from constant friction.
Flat feet cause the arch to collapse inward when standing and walking. This changes how weight is distributed across the entire foot and can create a muscle imbalance that results in the fifth toe rotating outward or inward over time.
Some people with flat feet develop a specific pattern where the fifth toe rotates outward because of the way the foot compensates during each step. Addressing the flat foot with orthotics or supportive footwear can sometimes slow or prevent further toe drift.
Osteoarthritis and rheumatoid arthritis both affect the joints of the foot, including the MTP joint of the fifth toe. Joint inflammation causes swelling, stiffness, and progressive changes in alignment.
Rheumatoid arthritis in particular is known to cause toe drift and deformity because it attacks the synovial tissue that lines the joints. As the joint is damaged, the structural support for the toe deteriorates and the toe begins to shift sideways.
A fracture, sprain, or dislocation of the fifth toe or fifth metatarsal bone can permanently alter alignment if not properly treated. Even an injury that heals without visible deformity can cause subtle changes in tendon tension or joint structure that lead to a gradual sideways drift later.
Stress fractures from repetitive activity — common in runners and dancers — can also weaken the metatarsal and change how the fifth toe is supported during movement.

Excess body weight places significant additional pressure on every part of the foot with each step. The forefoot and toes bear a disproportionate share of that load. Over time, the added stress can accelerate the development of deformities in the smaller toes, including the fifth.
Weight-related toe deformities tend to be progressive. Even a moderate reduction in body weight, combined with supportive footwear, can meaningfully reduce the mechanical load on the forefoot.
A sideways pinky toe is often noticed visually before it becomes painful. Knowing the associated symptoms helps gauge severity and urgency.
Common symptoms include:
Warning signs that require prompt medical attention:
A podiatrist typically diagnoses the condition through a combination of physical examination and imaging.
During the exam, the clinician will assess the toe’s range of motion, test whether it can be manually straightened (flexible vs. rigid), look for corns, calluses, or skin breakdown, and evaluate the overall alignment of the foot.
X-rays are the standard imaging tool for identifying bony changes, measuring the deviation angle of the metatarsal, and ruling out fractures. In some cases, gait analysis is performed to identify biomechanical patterns contributing to the toe’s position.
The large majority of sideways pinky toe cases can be managed without surgery, especially when caught early while the toe is still flexible.
The single most impactful non-surgical change is switching to shoes with a wide toe box. The toe box is the front section of the shoe where all the toes sit. A wide toe box allows the toes to spread naturally and eliminates the compressive force that drives misalignment.
Avoid narrow, pointed, or high-heeled shoes. Look for shoes with a rounded or square toe box, sufficient depth, and soft upper materials that do not press against the little toe.
Silicone or foam toe spacers are small devices placed between the toes to gently hold them apart and reduce friction. They can be worn inside shoes during the day or at night.
Toe spacers may help realign a flexible turned pinky toe over time by counteracting the inward pressure. They also provide immediate relief from the friction and rubbing that causes calluses and pain.
Taping the pinky toe back toward a natural position — or buddy taping it to the fourth toe for support — is a common conservative approach. This is particularly effective in babies and young children, where the toe is highly flexible and responds quickly to positional correction.
In infants with overlapping toes, consistent taping has shown very high success rates. One study found 94 percent of cases were cured or significantly improved within six months of starting taping therapy. Early treatment matters significantly.
Custom orthotics are shoe inserts prescribed by a podiatrist and made specifically for your foot’s shape and biomechanics. They redistribute pressure across the forefoot, correct overpronation, and reduce the mechanical forces that push the pinky toe out of alignment.
Off-the-shelf orthotics can also help with mild cases, particularly when flat feet or overpronation are contributing to the problem.
Targeted exercises improve flexibility and strengthen the intrinsic muscles of the foot, which play a key role in keeping the toes aligned. A podiatrist or physical therapist can design an appropriate routine.
Effective exercises for a sideways pinky toe:
These exercises are most effective when the toe is still flexible and the deformity has not become rigid.
Adhesive foam pads placed over a callus, bunionette, or sore spot on the fifth toe reduce friction and protect the skin while walking. This does not correct the underlying alignment but significantly reduces day-to-day discomfort.
Orthotic toe splints and wraps physically hold the fifth toe in a more aligned position, particularly during sleep when the foot is not bearing weight. They can slow the progression of the deformity and reduce tendon tightening over time.
When conservative treatments have failed, the toe has become rigid and fixed, or the pain significantly impacts daily life, surgery may be recommended.
Surgical options are tailored to the specific type and severity of the deformity. Common procedures include:
| Procedure | What It Does | Best For |
|---|---|---|
| Tendon release or transfer | Releases tight tendons or repositions them to restore balance | Flexible adductovarus deformity |
| Arthroplasty | Removes part of the bone at the bent joint to allow realignment | Hammertoe of the fifth toe |
| Osteotomy | Cuts and repositions the metatarsal bone | Tailor’s bunion / bunionette |
| Toe fusion (arthrodesis) | Permanently straightens and fuses the toe joint | Severe rigid deformity |
| Soft tissue repair | Tightens or repairs stretched ligaments and joint capsule | Joint instability |
Recovery time varies by procedure but generally involves a period of protected weight-bearing, followed by gradual return to activity over 4 to 8 weeks. Most patients experience significant pain relief and improved alignment after surgery.
A sideways pinky toe that goes untreated tends to worsen gradually. The longer it is left, the more likely the deformity becomes rigid and fixed — which significantly reduces the effectiveness of non-surgical treatment and may ultimately require more complex surgery.
Complications of an untreated sideways pinky toe:
Seeking evaluation early, when the toe is still flexible and moveable, offers the best outcome with the least invasive treatment.
A sideways or overlapping pinky toe in babies and young children is quite common and is often congenital — meaning the child was born with it. In infants, the fifth toe frequently overlaps the fourth toe due to the natural positioning in the womb.
The good news is that early intervention in infants and toddlers is highly effective. Consistent taping or manual stretching of the toe during the first year of life resolves the majority of cases without any further treatment.
The window for non-surgical correction narrows significantly once a child begins walking and the deformity starts to bear full body weight. Parents who notice a turned or overlapping pinky toe in an infant should consult a pediatric podiatrist promptly for the best chance of conservative correction.
Beyond specific treatments, a few everyday habits significantly reduce the risk of toe deformities developing or worsening.
Footwear checklist for pinky toe health:
Daily foot care habits:
Many people wait too long before seeking professional help for a sideways pinky toe, assuming it will resolve on its own. It rarely does. The toe tends to drift further over time without intervention.
See a podiatrist if:
A podiatrist will confirm the diagnosis, rule out fracture or arthritis, and guide you through the most appropriate treatment plan for your specific situation.
| Factor | Conservative Treatment | Surgical Treatment |
|---|---|---|
| Best for | Flexible, early-stage deformity | Rigid, fixed, or severe deformity |
| Recovery time | Days to weeks | 4 to 8 weeks |
| Effectiveness | High when caught early | High for advanced cases |
| Cost | Low to moderate | Higher |
| Risk | Minimal | Infection, stiffness, rare complications |
| Success rate | Good with compliance | Generally high |
 Frequently Asked Questions (FAQs)
Frequently Asked Questions (FAQs)A sudden change is usually caused by an injury, fracture, or a rapidly worsening tendon imbalance. See a podiatrist promptly if the shift happened suddenly, especially after trauma.
In adults, it very rarely corrects on its own. Without treatment the deformity typically progresses slowly. In infants, early taping therapy has a high success rate and can resolve the issue without surgery.
It is not dangerous on its own, but it can lead to corns, calluses, bursitis, skin breakdown, and gait changes if left untreated. People with diabetes need to take any toe deformity especially seriously.
The most common clinical term is adductovarus deformity of the fifth toe. It may also be called an overlapping fifth toe, underlapping fifth toe, or curly toe depending on how the toe is positioned.
Not always. Many cases are managed successfully with wide shoes, toe spacers, orthotics, and exercises. Surgery is typically only recommended when conservative measures fail or the toe becomes rigid and fixed.
A podiatrist is the primary specialist for this condition. In some cases, an orthopedic surgeon who specializes in foot and ankle care may also be involved, particularly if surgery is needed.
Yes. Narrow toe boxes and high heels are among the most common contributing factors. They compress the toes and force the fifth toe to rotate inward over time. Switching to wider shoes early can slow or halt the progression.
Results vary by severity and consistency of treatment. Mild flexible deformities may show improvement within weeks of using toe spacers and wider shoes. More pronounced cases can take several months of consistent conservative care.
Toe spreading, towel scrunching, marble pickups, and gentle manual stretching of the fifth toe are the most commonly recommended exercises. A podiatrist or physical therapist can design a tailored routine.
Yes. When the deformity causes pain, people naturally shift their gait to avoid loading the affected toe. These compensatory movement changes can create secondary pain in the ankle, knee, hip, or lower back over time.
Why is my pinky toe sideways is a question that often comes with more concern than people expect when they first notice the problem. The truth is that a turned fifth toe is one of the most common foot complaints, and it is also one of the most treatable — especially when addressed early.
Whether the cause is tight footwear, genetics, a tendon imbalance, a tailor’s bunion, or an old injury, the path forward usually starts with simple changes that cost very little.
Wide shoes, toe spacers, orthotics, and daily stretching exercises resolve the majority of mild to moderate cases without any surgical intervention. For rigid or severe deformities, modern surgical options offer highly effective correction with relatively short recovery times.
The key is not to wait. A flexible sideways pinky toe that is caught early is far easier to treat than one that has become stiff and fixed from years of neglect. If your little toe has started to drift, consult a podiatrist and take action now.