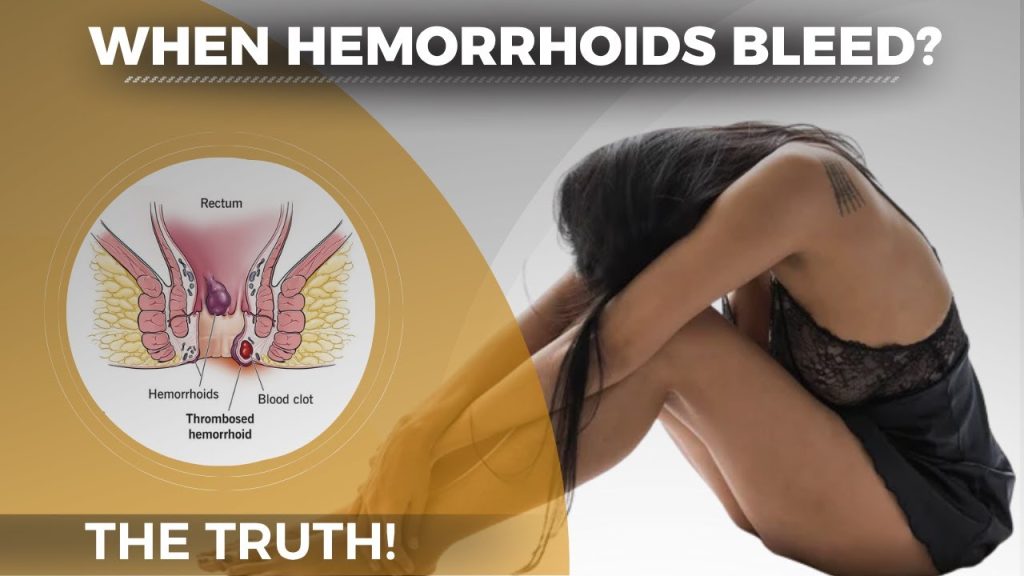
Why do hemorrhoids bleed? This is one of the most common questions people ask after noticing bright red blood on toilet paper or in the bowl.
Hemorrhoids are swollen veins in the rectum or anus that bleed when irritated, damaged, or ruptured by pressure.
The good news is that hemorrhoid bleeding is rarely dangerous and often manageable at home.
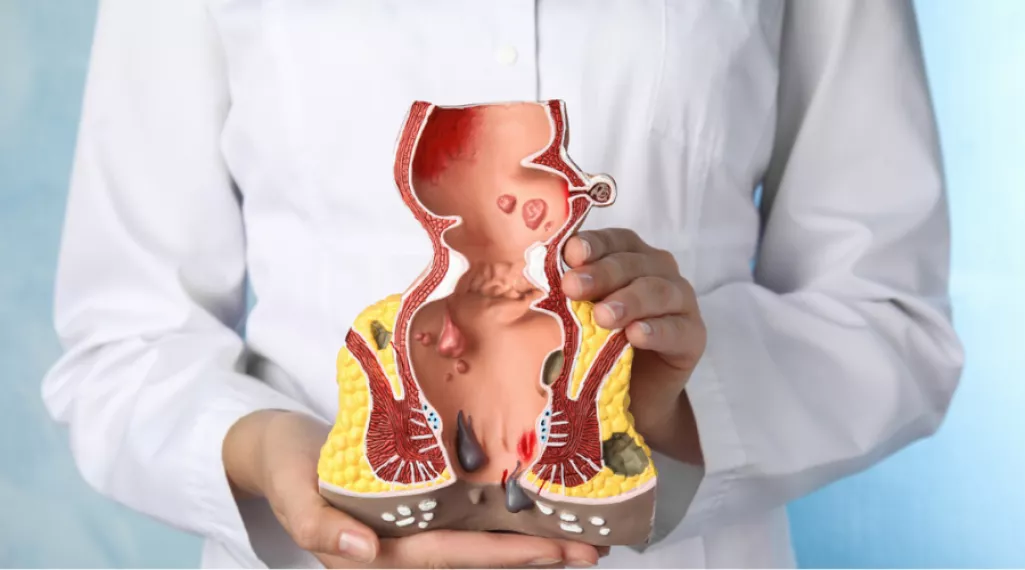
Hemorrhoids, also called piles, are cushion-like clusters of veins located in the lower rectum and around the anus. Everyone has hemorrhoidal tissue — it plays a role in bowel control. Problems begin when these veins become swollen, inflamed, or enlarged.
There are two main types:
The core reason hemorrhoids bleed comes down to vascular pressure and tissue damage. Here is what happens step by step:
Step 1 — Pressure builds. When you strain during bowel movements, the veins in the rectal area engorge with blood and swell under pressure.
Step 2 — Tissue thins. As internal hemorrhoids swell, the delicate tissue covering them becomes stretched and thin — almost like an overfilled balloon.
Step 3 — Rupture occurs. Hard stool passing through the rectum scrapes or ruptures these high-pressure vessel walls. Blood escapes, appearing as bright red blood on toilet paper, in the toilet bowl, or coating the stool.
Step 4 — Bleeding continues. Without lifestyle changes, the cycle repeats — more straining, more pressure, more bleeding.
This is why hemorrhoid bleeding looks bright red. The blood is fresh and comes from arteries and veins very close to the anal opening, not from deeper in the digestive system.
Understanding what triggers bleeding helps you address the root problem, not just the symptoms.
| Cause | How It Triggers Bleeding |
|---|---|
| Straining during bowel movements | Increases venous pressure, ruptures thin vessel walls |
| Chronic constipation | Produces hard stools that scrape hemorrhoid tissue |
| Chronic diarrhea | Repeated irritation weakens tissue |
| Prolonged toilet sitting | Applies direct downward pressure on rectal veins |
| Low-fiber diet | Leads to hard, dry stools |
| Dehydration | Makes stools harder and more abrasive |
| Pregnancy | Uterus pressure compresses rectal veins |
| Heavy lifting | Spikes intra-abdominal pressure suddenly |
| Obesity | Chronic pressure on pelvic veins |
| Aging | Vein walls weaken after age 50 |
Internal hemorrhoids are significantly more likely to bleed than external ones.
Internal hemorrhoids sit in a zone inside the rectum where pain-sensing nerves are sparse. This means they can bleed heavily without causing pain — which is why many people are shocked when they see blood but feel nothing.
External hemorrhoids bleed far less often. When they do bleed, it usually happens because they rupture or get irritated by aggressive wiping. External hemorrhoids are more commonly associated with pain, itching, and swelling.
Knowing what is normal versus alarming can save you unnecessary panic — or dangerous delays.
Normal hemorrhoid bleeding:
Warning signs that need a doctor:
Dark or maroon blood is not typical hemorrhoid bleeding. It points to a problem deeper in the gastrointestinal tract and requires prompt medical evaluation.
A few drops of bright red blood after a bowel movement is considered within the typical range for hemorrhoid-related bleeding.
Bleeding that soaks toilet paper, drips heavily into the bowl, or appears between bowel movements is not normal and warrants a doctor visit. Ongoing blood loss — even in small amounts — can accumulate over weeks and lead to iron-deficiency anemia.
Signs of anemia from hemorrhoid bleeding include:
If you notice any of these alongside rectal bleeding, see a specialist promptly.
Hemorrhoid bleeding linked to a single episode of constipation or hard stool often stops within a few days once the irritant is removed.
Bleeding that continues or keeps returning signals an underlying issue — usually ongoing straining, a poor diet, or untreated internal hemorrhoids that have grown large enough to bleed consistently.
If bleeding persists beyond 7 days despite home treatment, consult a healthcare provider.
Doctors use the Goligher classification system to grade internal hemorrhoids. Bleeding gets worse as the grade increases.
| Grade | Description | Bleeding Risk |
|---|---|---|
| Grade I | Small, no prolapse | Light, occasional bleeding |
| Grade II | Prolapse during straining, returns on its own | Moderate, recurring bleeding |
| Grade III | Prolapse, must be pushed back manually | Frequent bleeding |
| Grade IV | Permanent prolapse, cannot be reduced | Heavy or constant bleeding |
Grade I and II hemorrhoids typically respond well to home treatment. Grade III and IV often need medical procedures.

Most mild hemorrhoid bleeding can be managed at home with a focused plan. Here are the most effective options:
Fill a shallow basin or your bathtub with a few inches of warm water — around 104°F (40°C). Soak your hips and buttocks for 15 to 20 minutes. Do this two to three times daily, especially after bowel movements.
Warm water relaxes the internal anal sphincter, reduces swelling, and keeps the area clean so irritated tissue can heal. This is one of the most consistently recommended treatments across medical sources.
Apply an ice pack wrapped in a thin cloth to the anal area for 10 minutes. Cold constricts blood vessels and slows active bleeding.
Do not apply ice directly to skin. Limit cold application to 10-minute sessions to avoid tissue damage.
Fiber softens stools and reduces the straining that causes hemorrhoids to rupture. The recommended daily target is about 28 grams for a 2,000-calorie diet.
High-fiber foods to add to your plate:
If food is not enough, psyllium-based supplements like Metamucil are well-supported by research. Increase fiber gradually to avoid bloating.
Drink at least 8 glasses of water daily. Dehydration hardens stools, making every bowel movement a potential trigger for hemorrhoid bleeding.
Water is the simplest and cheapest fix in your toolkit. Pair it with fiber for maximum effect.
Aggressive, dry wiping is one of the most overlooked causes of repeated hemorrhoid bleeding. Switch to unscented moist wipes or damp toilet paper. Pat gently — do not rub.
Sitting on a standard toilet puts downward pressure on the rectal veins. A small footstool that raises your knees above hip level mimics a squatting position and reduces straining pressure significantly.
Limit toilet time to under 5 minutes. Leave your phone outside the bathroom.
Several OTC products can reduce inflammation and shrink swollen tissue:
| Product Type | Key Ingredients | What They Do |
|---|---|---|
| Topical creams | Hydrocortisone, witch hazel, pramoxine | Reduce inflammation and numb the area |
| Suppositories | Phenylephrine, hydrocortisone | Shrink internal hemorrhoid tissue |
| Fiber supplements | Psyllium, methylcellulose | Soften stools to prevent straining |
| Stool softeners | Docusate sodium | Reduce stool hardness |
| Sitz bath additives | Epsom salts, baking soda | Soothe irritated tissue |
Do not use hydrocortisone products for more than 7 days consecutively without a doctor’s guidance. Prolonged steroid use can thin the skin and worsen the condition.
When home remedies are not enough, doctors have several effective non-surgical and surgical options.
A small rubber band is placed at the base of the hemorrhoid to cut off its blood supply. The hemorrhoid shrinks and falls off within 7 to 10 days. This is the most commonly performed office procedure for internal hemorrhoid bleeding and has a high success rate.
A doctor injects a chemical solution directly into the hemorrhoid. This creates scar tissue that cuts off blood flow and shrinks the hemorrhoid. It is a good option for patients who are on blood thinners or cannot tolerate banding.
Infrared light heat is applied to the base of the hemorrhoid to seal blood vessels and reduce blood supply. Multiple sessions may be needed for significant results.
An electric probe creates a small burn that seals the end of the hemorrhoid and causes it to close off and shrink. Works well for prolapsed hemorrhoids.
This is a newer, minimally invasive procedure performed by an interventional radiologist. A microcatheter is navigated to the superior rectal artery and microspheres are deployed to reduce arterial blood flow to the hemorrhoids. It is suitable for patients with high surgical risk and allows quick recovery with minimal discomfort.
Surgical removal of the hemorrhoid. This is reserved for Grade III–IV hemorrhoids, large external hemorrhoids, or cases that have failed all other treatments. Recovery involves significant post-operative pain but has a very low recurrence rate.
Diet plays a central role in hemorrhoid management. Here is a practical breakdown:
Foods to eat more of:
Foods to limit or avoid:
Dietary changes take 2 to 4 weeks to show a significant difference in hemorrhoid symptoms. Consistency is the key.
Treating an episode of bleeding is one thing. Preventing the next one is another. These habits address the root causes:
Exercise regularly. Physical movement stimulates healthy digestion and prevents constipation. A 30-minute walk most days is enough to make a difference.
Never delay bowel movements. Stool gets harder and drier the longer it stays in the colon. Go when you feel the urge.
Avoid heavy lifting. Sudden spikes in intra-abdominal pressure can aggravate hemorrhoids. If you must lift, breathe out during exertion rather than holding your breath.
Maintain a healthy weight. Excess body weight puts chronic pressure on pelvic veins, increasing hemorrhoid risk.
Avoid prolonged sitting. If your job requires sitting for long periods, stand up and walk for a few minutes every hour.
Not all rectal bleeding is harmless. See a doctor if:
Rectal bleeding is the most commonly missed opportunity to diagnose colorectal cancer early. Do not assume it is always hemorrhoids.
Hemorrhoids are very common during pregnancy because the growing uterus compresses the rectal veins, hormonal changes affect vein elasticity, and constipation is frequent.
Safe management options during pregnancy include:
Most pregnancy-related hemorrhoid bleeding resolves after delivery. If symptoms are severe or bleeding does not improve within a few days, consult your healthcare provider.
Yes. While a single episode of hemorrhoid bleeding rarely causes anemia, repeated or chronic blood loss can lead to iron-deficiency anemia over time.
This is more common with Grade III and IV internal hemorrhoids that bleed consistently during bowel movements. If you feel persistently tired, dizzy, or short of breath alongside ongoing rectal bleeding, ask your doctor for a blood count test.
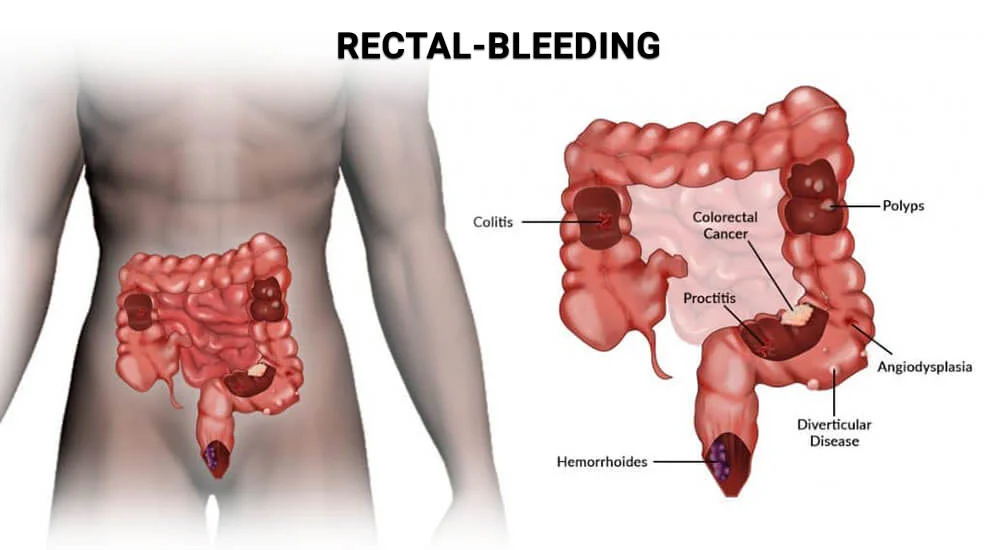
Not every instance of rectal bleeding comes from hemorrhoids. Other conditions that can cause blood in stool include:
| Condition | Blood Appearance | Other Symptoms |
|---|---|---|
| Hemorrhoids | Bright red, on surface of stool or toilet paper | Itching, anal discomfort |
| Anal fissure | Bright red, often with pain | Sharp pain during bowel movements |
| Colorectal cancer | Bright or dark red, mixed in stool | Weight loss, bowel habit changes |
| Diverticular disease | Bright or dark red, often painless | Abdominal cramps |
| IBD (Crohn’s, Colitis) | Dark or bright red, mixed in stool | Diarrhea, cramps, fever |
| Anal fistula | Bright red with discharge | Persistent anal pain or drainage |
Hemorrhoid diagnosis is clinical — your doctor can usually confirm it with a physical exam and digital rectal exam. A colonoscopy may be recommended if there are any red flags.
Internal hemorrhoids form above the dentate line, where pain-sensing nerves are absent. They bleed easily from vascular pressure without triggering pain signals, which is why many people are surprised to see blood and feel nothing at all.
Most hemorrhoid bleeding is minor and self-limiting. However, chronic blood loss can cause iron-deficiency anemia, and rectal bleeding can sometimes signal more serious conditions like colorectal cancer that require investigation.
Apply gentle pressure with clean gauze, follow up with an ice pack for 10 minutes, and take a warm sitz bath. Avoid straining and increase fiber and water intake to prevent recurrence.
Go to the ER if you experience heavy, uncontrolled rectal bleeding, blood mixed with dizziness or fainting, or bleeding accompanied by severe abdominal pain and fever.
Yes, though it is less common. Prolapsed or thrombosed hemorrhoids can bleed spontaneously. Any bleeding outside of bowel movements should be evaluated by a doctor.
Hemorrhoid blood is always bright red. Dark red, maroon, or black blood points to bleeding higher up in the digestive tract and requires immediate medical attention.
Minor bleeding caused by a single irritation often stops within 1 to 3 days. Recurring or persistent bleeding linked to untreated internal hemorrhoids can continue indefinitely without medical treatment.
Stress does not directly cause hemorrhoid bleeding, but it can lead to habits — like ignoring the urge to defecate, poor diet, or reduced physical activity — that worsen constipation and increase hemorrhoid flare-ups.
Yes. Adequate hydration softens stools, reducing the straining that causes hemorrhoid vessels to rupture. Aim for at least 8 glasses of water per day alongside a high-fiber diet.
Grade I and II hemorrhoids often improve significantly with dietary and lifestyle changes. Grade III and IV hemorrhoids typically require medical intervention and are unlikely to resolve fully on their own.
Why do hemorrhoids bleed? The answer is simple: pressure, fragile vein walls, and irritation from hard stools or straining cause these swollen vessels to rupture during bowel movements.
While the sight of bright red blood can be alarming, most hemorrhoid bleeding is manageable with the right approach. Start with fiber, hydration, sitz baths, and better toilet habits. Use OTC creams for short-term symptom relief.
If bleeding persists beyond a week or is heavy and recurring, see a specialist — procedures like rubber band ligation are quick, effective, and far less daunting than most people expect.
Most importantly, never ignore rectal bleeding. Get a proper diagnosis, rule out other causes, and take early action to protect your long-term health.