Why is my knee so tight after meniscus surgery is one of the most searched questions during post-op recovery, and for good reason.
That wrapped, rubber-band feeling in your knee is real, it is frustrating, and it can last for weeks or even months.
The good news is it is almost always explainable and manageable.

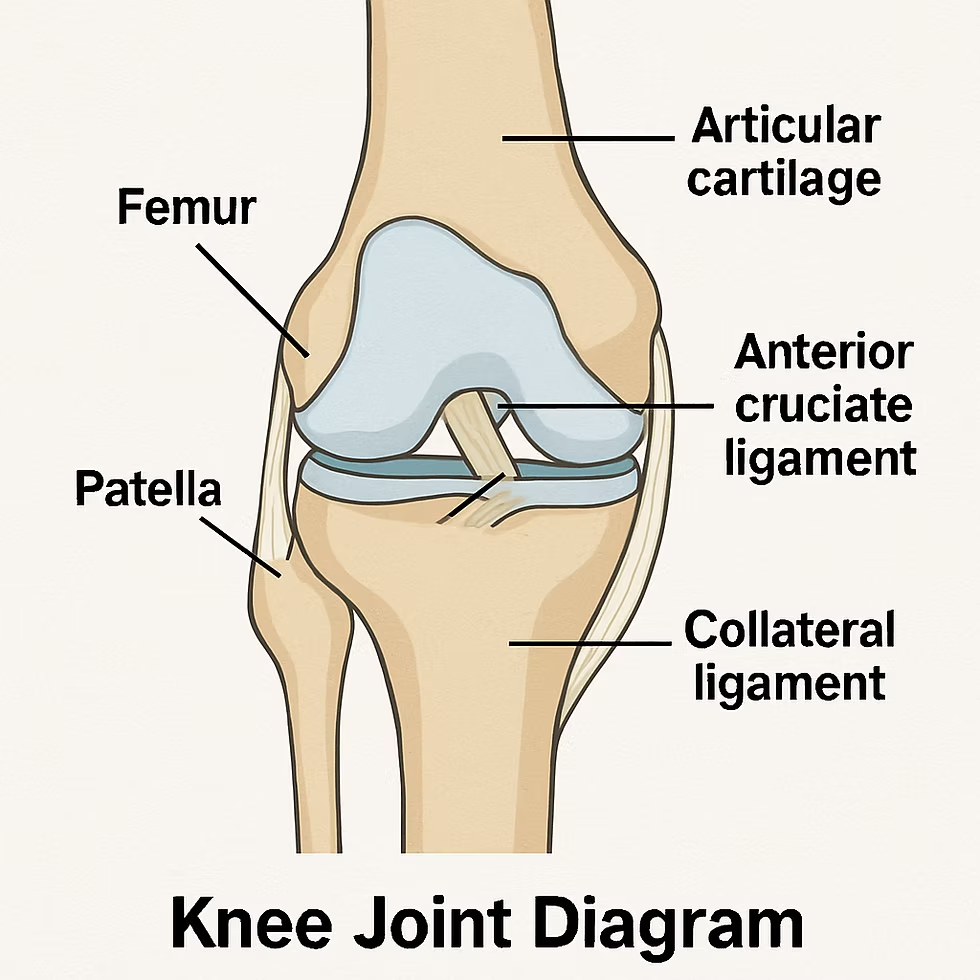
The meniscus is a C-shaped piece of cartilage sitting between your thigh bone (femur) and shin bone (tibia) in each knee. It acts as a shock absorber, distributes load across the joint, and keeps the knee stable during movement.
When it tears, surgery is often needed. Either the surgeon removes the damaged portion (partial meniscectomy) or stitches the tissue back together (meniscus repair). Both procedures disturb the joint enough to trigger a significant healing response, and that healing response is the root cause of tightness.
Knowing which surgery you had helps set realistic expectations for tightness and recovery.
| Surgery Type | What Happens | Recovery Timeline | Tightness Duration |
|---|---|---|---|
| Partial Meniscectomy | Damaged portion removed | 4 to 6 weeks typical | 2 to 6 weeks common |
| Meniscus Repair | Torn tissue stitched back | 4 to 6 months | Up to 3 to 4 months possible |
| Complex Repair | Multiple sutures, larger tear | Up to 6+ months | Several months with PT |
Meniscus repair patients experience longer and more intense tightness because the knee is immobilized longer to allow the stitched tissue to heal without stress.
There is never just one reason. Multiple factors typically combine to create that tight, stiff sensation in your knee.
Swelling is the body’s first response to any surgical trauma. Blood flow increases, fluid rushes to the area, and the joint becomes congested. This excess fluid physically compresses the joint space, limiting how far you can bend or straighten the knee.
Studies show that around 25 percent of patients report significant stiffness after knee surgeries due to ongoing swelling. The inflammation alone can restrict range of motion for several weeks.
After any surgery, the body lays down fibrous tissue as part of the repair process. Inside and around the knee joint, this scar tissue can form adhesions that literally glue structures together, limiting smooth movement.
Research indicates up to 10 percent of patients develop lasting stiffness from excessive scar tissue buildup. Physical therapy targets this directly by mobilizing the tissue before it fully matures and hardens.
After surgery, muscles surrounding the knee contract involuntarily to protect the joint. This protective tension, called muscle guarding, is an automatic reflex. Your quadriceps, hamstrings, and calf muscles tighten around the knee to brace it.
While helpful immediately after surgery, prolonged muscle guarding becomes a source of stiffness itself. It limits joint movement even when the underlying injury is healing well.
Arthrofibrosis is a more serious condition where excessive fibrous tissue forms inside the joint itself, not just around it. It causes significant and persistent tightness that does not resolve with standard rest and home exercises.
Signs of arthrofibrosis include tightness that does not improve with weeks of consistent physical therapy, inability to fully straighten or bend the knee, and pain that feels worse rather than better over time.
When part of the meniscus is removed or repaired, the way forces travel through the knee changes. The joint surfaces can become irritated, and that irritation produces chronic stiffness, especially the classic morning stiffness and tightness after sitting for long periods.
This is one of the documented reasons why meniscectomy is linked to accelerated cartilage changes in the long term.
After meniscus repair, the knee is often kept in a brace and movement is heavily restricted for four to six weeks. Immobilization causes muscles to weaken and joint structures to stiffen rapidly. When rehabilitation begins, the joint has to work hard to regain the range of motion it lost during the rest period.
Even after a meniscectomy, reduced daily activity in the first weeks contributes to stiffness as muscles and soft tissues adapt to a lower movement demand.
Starting physical therapy too late, skipping sessions, or following a generic program that does not address your specific joint condition can all allow scar tissue to mature and tighten. The window for effective scar tissue intervention is narrower than most people realize.
Scar tissue that is three months old responds well to manual therapy and mobilization. Scar tissue that is twelve months old is far harder to change.

Normal post-surgical tightness has certain recognizable patterns. Understanding what is typical helps you avoid unnecessary panic.
Many patients describe their knee as feeling like it is wrapped in a tight rubber band. This reflects the combination of swelling, capsular tension, and scar tissue around the joint.
It is most intense in the first two to four weeks and should gradually ease with consistent movement and therapy.
Waking up with a stiff knee that loosens after the first ten to fifteen minutes of movement is very common and is generally normal during recovery. Fluid pools in the joint during rest and needs to be pumped back through movement.
If morning stiffness lasts longer than thirty minutes or progressively gets worse rather than better, consult your surgeon.
Tightness that returns every time you sit for more than twenty or thirty minutes is another common pattern. The knee settles into a bent position, fluid accumulates, and straightening it again requires effort and brief discomfort.
This stiffness pattern usually improves significantly by weeks six to eight of rehabilitation.
Inability to fully extend the knee (straightening it completely flat) is one of the most important symptoms to address early. Failing to regain full extension leads to chronic pain, altered walking gait, and accelerated arthritis over time.
If you cannot straighten your knee to match the other side within a few weeks of starting therapy, tell your physical therapist immediately.
| Phase | Timeframe | What to Expect |
|---|---|---|
| Early Recovery | Weeks 0 to 2 | Significant swelling, limited bend and straighten, protected weight bearing |
| Early Rehab | Weeks 2 to 6 | Swelling reducing, basic range of motion exercises, crutches phased out |
| Active Rehab | Weeks 6 to 12 | Feeling more normal, strength and balance training, stiffness improving |
| Return to Activity | Weeks 12 to 24+ | Low-impact sports possible, most tightness resolved with good PT |
| Full Recovery (Repair) | 4 to 6 months | Full bending expected, sports return depends on surgeon clearance |
For a partial meniscectomy, full recovery typically takes four to five months. For a meniscus repair, it can take six months or longer for complex cases.
Exercise is the single most effective tool for fighting post-surgical knee tightness. Always follow your physical therapist’s guidance on timing and progression.
Lie flat on your back. Slowly slide your heel toward your buttocks, bending the knee as far as comfortable. Hold for five seconds. Slowly straighten. This gently increases flexion range without loading the joint.
Start with ten repetitions two to three times daily in the first week or two post-surgery.
Lie with your leg flat on the floor. Tighten your thigh muscle (quadriceps) as if pushing the back of your knee into the floor. Hold for five seconds, then relax. This activates the quad without bending the knee.
This is often the very first exercise prescribed after surgery because it prevents muscle wasting and helps maintain joint extension.
Tighten your quad, then lift your straight leg to about 45 degrees. Hold briefly, lower slowly. This strengthens the quadriceps and hip flexors without any knee joint compression.
Progressing quad strength is essential because the quad is the primary stabilizer of the knee during walking.
Sit in a chair and place your heel on a surface of the same height. Let gravity gently pull your knee toward full extension. Do not force it. Hold for ten to fifteen minutes.
Recovering full extension is the number-one priority in the first weeks of rehabilitation. This passive stretch helps regain it without overloading the joint.
Move your foot up and down repeatedly, pumping the calf muscle. This sounds simple but it actively pumps fluid out of the lower leg and knee, reducing swelling and the stiffness that comes with it.
Do this frequently throughout the day, especially during the first two weeks when swelling is highest.
Lie face down. Slowly try to bend your knee, bringing your heel toward your buttocks. Use a towel looped around your ankle to gently assist the stretch if needed. Hold at the edge of comfortable range for twenty to thirty seconds.
This helps regain flexion range and stretches the quadriceps at the same time.
Place a rolled towel under your knee. Tighten the quad and straighten the lower leg fully. Hold two seconds, then slowly lower. This exercises the terminal range of knee extension, which is often the hardest part of motion to recover.
Physical therapy is not optional if you want to resolve knee tightness and regain full function. Research from the American Physical Therapy Association recognizes manual therapy combined with targeted exercise as the gold standard for post-surgical knee rehabilitation.
A skilled physical therapist performs hands-on techniques to mobilize the kneecap (patellar mobilization), stretch the joint capsule, and break down early scar tissue. These techniques cannot be replaced by doing exercises alone.
If your PT program consists only of exercises with minimal hands-on time, advocate for more direct manual work.
The kneecap (patella) can become restricted after knee surgery, contributing significantly to tightness. Your therapist should check patellar mobility and mobilize it in all directions if it is restricted.
A stuck kneecap makes bending and straightening the knee much harder than it should be.
Physical therapy appointments are typically scheduled twice a week for six to eight weeks after meniscectomy, and for several months after meniscus repair. Attending consistently makes a measurable difference in how quickly tightness resolves.
Skipping sessions allows scar tissue to organize and harden between visits, undoing progress.
Certain common mistakes prolong tightness and delay recovery.
There is a difference between the productive discomfort of stretching a stiff joint and sharp, stabbing pain that signals tissue damage. Never force a stiff knee past a point of sharp pain. Work to the edge of comfortable stiffness and hold there.
Immobility is one of the biggest drivers of worsening stiffness. Even gentle movement, ankle pumps, and quad sets while sitting help prevent fluid pooling and scar tissue organization.
Unless your surgeon has specifically told you not to move, gentle motion is almost always beneficial.
Ice therapy remains valuable throughout early and mid recovery. After exercises, apply an ice pack wrapped in a cloth to the knee for fifteen to twenty minutes. This manages the temporary inflammation that exercise creates.
Do not apply ice directly to skin. Always use a cloth barrier.
Returning to running, jumping, or sport before your surgeon and therapist clear you significantly increases the risk of re-tear and causes a fresh inflammatory response that sets back your stiffness recovery.
Most patients return to low-impact sports around four to five months post-surgery and high-impact sports only when fully cleared.
Most knee tightness after meniscus surgery is expected. However, some signs indicate a complication that needs prompt medical attention.
| Warning Sign | Possible Cause |
|---|---|
| Sudden increase in swelling and heat | Infection or blood clot (DVT) |
| Fever alongside knee swelling | Surgical site infection |
| Tightness not improving after 3 months with PT | Arthrofibrosis |
| Knee locking and clicking that worsens | Failed repair or loose fragment |
| Inability to bear any weight | Re-tear or structural failure |
| Redness, discharge from incision | Wound infection |
| Persistent numbness or tingling | Nerve involvement |
Contact your surgeon immediately if you experience any of the above. Do not wait for your next scheduled appointment.
Arthrofibrosis deserves its own section because it is underdiagnosed and can cause lasting disability if not addressed early.
It develops when the body’s healing response overproduces fibrous tissue inside the joint capsule. The knee becomes progressively less mobile despite exercise. It affects an estimated 10 percent of patients following knee surgery.
The key signs are tightness that does not respond to physical therapy after six to twelve weeks, inability to reach 90 degrees of bend, significant loss of extension, and pain that worsens rather than plateaus.
Early arthrofibrosis responds well to aggressive physical therapy, intensive manual mobilization, and anti-inflammatory medications. Your doctor may recommend a corticosteroid injection to reduce inflammation inside the joint.
In resistant cases, a procedure called manipulation under anesthesia (MUA) is performed. The surgeon manually breaks up the scar tissue while you are under anesthesia. In severe cases, arthroscopic surgery to physically remove the scar tissue may be necessary.
Body weight, diet, and daily habits all influence how quickly your knee loosens up after surgery.
Excess body weight places additional compressive force on the healing knee joint with every step. Even a modest reduction in weight during recovery reduces joint load and can speed up the return of comfortable range of motion.
Overweight patients also tend to develop more intense swelling after surgery, which prolongs tightness.
Consuming foods rich in omega-3 fatty acids (salmon, walnuts, flaxseed), colorful vegetables, and antioxidants supports the body’s ability to modulate the inflammatory response. Reducing processed foods, sugar, and alcohol during recovery is also beneficial.
This does not replace medical treatment, but it creates a better internal environment for healing.
Tissue repair happens primarily during deep sleep. Prioritizing seven to nine hours of sleep per night, elevating the leg when resting, and avoiding prolonged periods of sitting with the knee completely bent all contribute to better recovery outcomes.
When tightness is severe or not responding to physical therapy, your doctor has additional tools available.
An injection of corticosteroid medication directly into the knee joint reduces inflammation rapidly. It typically begins working within two to three days and can significantly reduce swelling-driven tightness, making it easier to progress in physical therapy.
Corticosteroids are usually given only once due to the risk of cartilage effects with repeated use.
Sometimes called viscosupplementation, hyaluronic acid injections lubricate the joint, reducing friction and improving the smoothness of movement. These are more commonly used for arthritis-related tightness but can sometimes help post-surgical stiffness.
For chronic scar tissue and tendinopathy that has not responded to standard physical therapy, shockwave therapy applies acoustic waves to the tissue to stimulate breakdown and remodeling. It is typically a self-pay service but can produce real change when standard care has plateaued.
What you do between physical therapy appointments matters just as much as the sessions themselves.
Keep the leg elevated above heart level as much as possible during the first two to four weeks. This reduces swelling passively by using gravity to drain fluid away from the knee.
Use pillows to prop the entire leg, not just the foot, so the knee itself is elevated.
A compression bandage or knee sleeve reduces swelling by providing gentle external pressure on the joint. Wear it during the day, especially when active, but remove it at night to allow circulation during sleep.
Ice is best in the first two to three weeks when inflammation and acute swelling are the dominant issue. After the initial inflammatory phase, heat therapy can be used before stretching exercises to warm the soft tissue and make it more pliable.
Do not use heat when the knee is acutely swollen or warm to the touch.
| Therapy | When to Use | Duration |
|---|---|---|
| Ice | Acute swelling, after exercise | 15 to 20 minutes |
| Heat | Before stretching, stiffness after acute phase | 10 to 15 minutes |
| Elevation | Any time while resting | As long as comfortable |
| Compression | During activity, daytime use | Remove at night |
Even on non-PT days, performing your home exercise program consistently is essential. Gentle range-of-motion exercises twice daily keep fluid moving and prevent scar tissue from organizing overnight.
Think of it as maintenance: you are not undoing damage, you are preventing new stiffness from setting in.
Patients recovering from a meniscectomy and a meniscus repair have significantly different experiences with tightness.
After a meniscectomy, weight bearing is often allowed immediately or within days. Physical therapy typically begins within the first week. Most patients notice significant improvement in tightness by four to six weeks, with full range of motion returning by three to four months.
After a meniscus repair, the knee is braced and movement is restricted for up to six weeks to protect the stitched tissue. This immobilization creates more intense and longer-lasting tightness. Rehabilitation is more gradual, and full recovery takes four to six months or longer.
Both types of surgery require consistent physical therapy. The meniscus repair patient simply needs more patience with the process.
Living with a tight, stiff knee for months is mentally exhausting. Fear of re-injury often causes patients to guard the knee subconsciously, which worsens muscle tension and stiffness.
Understanding that movement, done correctly, helps rather than harms the healing knee is an important mental shift. Your physical therapist should explain what each exercise is doing and why, so that you trust the process of loading the joint.
Anxiety about pain during exercises is very common. Discuss it openly with your PT. Knowing the difference between productive discomfort and harmful pain makes it much easier to commit to the rehabilitation process.
After a meniscectomy tightness typically improves within four to six weeks with physical therapy. After a repair it can last three to four months or longer.
Yes. Swelling, scar tissue formation, and muscle guarding are all expected parts of healing and all contribute to that tight sensation in the knee.
Full extension should return within the first few weeks of physical therapy. Persistent inability to straighten the knee needs to be addressed urgently with your PT and surgeon.
A temporary increase in swelling and inflammation after exercise is normal and usually settles within a few hours. Apply ice for fifteen to twenty minutes after each session.
Arthrofibrosis is excessive scar tissue formation inside the joint that prevents normal movement. It affects about 10 percent of patients and needs aggressive early treatment to prevent lasting stiffness.
Use ice in the first two to three weeks when swelling is active. Switch to heat before stretching once the acute swelling phase has passed to improve tissue flexibility.
Walking with a tight knee is generally safe and encouraged as tolerated after a meniscectomy. After a repair, follow your surgeon’s specific weight-bearing instructions carefully.
Persistent tightness beyond three months despite consistent therapy may indicate arthrofibrosis, inadequate rehabilitation, a failed repair, or early joint degeneration. See your surgeon for evaluation.
Consistent daily home exercises, attending all PT sessions, controlling swelling with ice and elevation, and maintaining a healthy weight all accelerate recovery significantly.
Call if tightness is worsening rather than improving, if you develop sudden swelling with heat and redness, if you cannot bear weight, or if tightness does not improve at all after six to eight weeks of physical therapy.
Why is my knee so tight after meniscus surgery is one of the most common questions in orthopedic recovery, and the answer involves multiple overlapping factors: post-surgical swelling, scar tissue formation, muscle guarding, changed joint mechanics, and in some cases arthrofibrosis.
The tightness is real, but in the vast majority of cases it is also temporary and treatable.
The single most important thing you can do is commit fully to physical therapy, attend every session, and perform your home exercises consistently between appointments.
Do not push through sharp pain, but do not let fear of discomfort stop you from moving.
Keep the knee elevated, manage swelling with ice in the early weeks, and use heat before stretching once the acute phase passes.
Monitor for warning signs that suggest a complication, and never hesitate to contact your surgeon if something feels wrong.
With the right approach, most patients recover full or near-full range of motion and return to the activities they love.