
Why does the bottom of my foot hurt is one of the most common questions people type into a search bar after waking up with that sharp, stabbing heel pain or a deep ache through the arch.
The bottom of the foot bears your entire body weight with every step, making it one of the most stressed structures in your body. Pain in this area can range from a mild soreness after a long day on your feet to a chronic, debilitating condition that affects your quality of life.
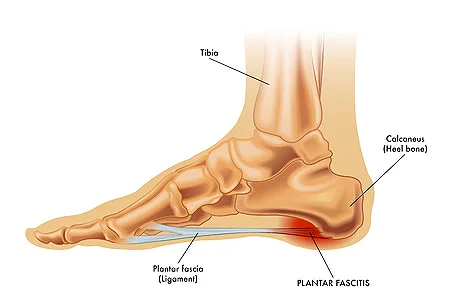
Before diving into causes, it helps to understand what is actually inside the bottom of your foot. The sole contains bones, tendons, ligaments, nerves, fat pads, and fascia all working together.
The plantar fascia is the thick fibrous band that runs from your heel bone to the base of your toes. It forms the arch, absorbs shock, and supports your foot with every step. When any part of this complex structure becomes damaged or inflamed, you feel it immediately.
The bottom of the foot is divided into three main zones: the heel (hindfoot), the arch (midfoot), and the ball of the foot (forefoot). Pain in each zone typically points to a different set of conditions.
| Pain Location | Most Likely Causes |
|---|---|
| Heel, worst in the morning | Plantar fasciitis, heel spurs |
| Middle of the arch | Flat feet, plantar fasciitis, tendinitis |
| Ball of the foot | Metatarsalgia, Morton’s neuroma, sesamoiditis |
| Burning or tingling throughout | Peripheral neuropathy, tarsal tunnel syndrome |
| Painful growth or bump | Plantar wart, corn, callus |
| Sudden pain after impact | Stress fracture, bruised fat pad |
| Pain all over the sole | Arthritis, overuse injury, diabetes-related |
Use this table as a starting point. A proper diagnosis from a podiatrist or orthopedic specialist is always the best path forward.
Plantar fasciitis is the single most common cause of pain on the bottom of the foot. It affects millions of adults every year and is the leading driver of heel pain in the general population.
It happens when the plantar fascia — the thick ligament-like band running across the sole — becomes inflamed from overuse, tight calf muscles, poor footwear, or a sudden increase in activity. The result is a sharp, stabbing pain concentrated at the heel or along the arch.
The defining symptom is pain that is worst during the first few steps after waking up or after sitting for a long period. The pain tends to ease once you start moving but can return after prolonged standing or at the end of the day.
Women are more likely to develop plantar fasciitis than men. People who are overweight, those who stand on hard surfaces for work, runners, and anyone with flat feet or high arches are at elevated risk.
Tight calf muscles are a major contributing factor. When the calf is tight, it pulls on the Achilles tendon, which in turn increases strain on the plantar fascia attachment point at the heel.
Rest and reduce high-impact activity in the short term. Ice the heel for 20 minutes three times per day to reduce inflammation — apply to the heel and arch, not the toes.
Stretch your calf muscles and the plantar fascia consistently every morning before you take your first steps. A tight calf is one of the most overlooked drivers of this condition.
Wear supportive shoes with good arch support at all times. Going barefoot on hard floors dramatically worsens plantar fasciitis. Night splints, custom orthotics, and physical therapy are effective next steps if home treatment does not improve symptoms within two weeks.
A heel spur is a bony growth that develops on the underside of the heel bone, typically at the point where the plantar fascia attaches. It forms over time as the body’s response to repeated stress and inflammation at that attachment site.
Heel spurs themselves do not always cause pain. Many people have them on X-rays with no symptoms at all. However, when they aggravate the surrounding soft tissue or co-exist with plantar fasciitis, they can produce sharp pain during weight-bearing activity.
Conservative treatment mirrors plantar fasciitis management: rest, ice, anti-inflammatory medication, and supportive footwear. Heel cushion inserts placed inside the shoe can reduce direct pressure on the spur and provide immediate relief.
Corticosteroid injections are used when pain is persistent and does not respond to several weeks of home care. Surgery to remove the spur is rarely necessary and is only considered after all other options have been exhausted.
Metatarsalgia refers to pain and inflammation in the ball of the foot — the area just behind the toes on the sole. The name comes from the metatarsal bones, which are the long bones connecting the ankle area to the toes.
The pain can feel sharp, aching, or burning and is typically made worse by standing, walking, running, or flexing the foot. Many people describe it as feeling like they are walking with a pebble stuck in their shoe.
High-impact sports, ill-fitting shoes (especially high heels or shoes with a narrow toe box), excess body weight, and foot deformities such as hammertoes or bunions are the most common causes.
Switch to shoes with better cushioning and a wider toe box immediately. Metatarsal pads and shock-absorbing insoles can redistribute pressure away from the painful area and offer quick relief.
Rest from high-impact activities like running and jumping. Ice the ball of the foot for 15-20 minutes several times per day. Over-the-counter NSAIDs such as ibuprofen help reduce inflammation and pain in the short term.

Morton’s neuroma is a thickening of the tissue around one of the nerves running to your toes, most commonly between the third and fourth toes. It causes a sharp, burning pain in the ball of the foot, often with numbness or tingling in the toes.
Many people with Morton’s neuroma describe the sensation as stepping on a small marble or folded sock inside their shoe. The pain is typically worst when wearing tight or narrow shoes and improves when you take your shoes off and rest.
High heels, shoes with a narrow toe box, and activities that put repetitive pressure on the forefoot are the most common triggers. Women are significantly more likely to develop this condition than men.
Switching to wider, lower-heeled shoes with plenty of toe room is the first and most important step. Metatarsal pads placed just behind the ball of the foot can relieve the nerve compression that causes symptoms.
If conservative measures do not resolve symptoms after several weeks, a podiatrist may recommend corticosteroid injections to reduce inflammation around the nerve. In persistent or severe cases, surgical removal of the neuroma or decompression of the nerve is considered.
Flat feet, also called fallen arches, occur when the arch of the foot collapses and the entire sole makes contact with the ground. This alters how forces are distributed through the foot, ankle, and knee with every step.
Flat feet do not always cause pain. However, when they do, the pain is typically felt along the inner arch, the heel, or even up into the ankle and lower leg. People with flat feet often develop overpronation — an inward rolling of the foot — which creates additional strain on the plantar fascia and tendons.
Supportive footwear with built-in arch support is the foundation of flat foot management. Motion-control running shoes are specifically designed for people with flat feet and overpronation.
Custom orthotics prescribed by a podiatrist provide a higher level of support and correction than off-the-shelf insoles. Physical therapy exercises that strengthen the foot’s intrinsic muscles and the posterior tibial tendon can improve arch support over time.
Peripheral neuropathy is damage to the nerves outside the brain and spinal cord. In the feet, it typically causes burning, tingling, numbness, or sharp electric-shock sensations on the bottom of the foot.
Diabetes is the most common cause of peripheral neuropathy in the feet. High blood sugar levels damage nerve fibers over time, particularly in the feet and lower legs. Other causes include alcohol misuse, vitamin B12 deficiency, certain medications, and inherited conditions.
Symptoms of neuropathy are often worse at night and can significantly disrupt sleep. The loss of sensation that accompanies neuropathy can make it harder to detect pressure points or injuries, putting the feet at risk of developing sores and ulcers.
Managing the underlying condition — especially blood sugar control in diabetes — is the most effective long-term solution. People with diabetic neuropathy must inspect their feet daily for any cuts, blisters, or pressure sores that they may not feel.
Wear compression socks to improve circulation. Soak feet in warm Epsom salt for 20 minutes daily to reduce discomfort. Topical treatments containing lidocaine or capsaicin can numb the area temporarily. Prescription medications such as gabapentin or pregabalin are commonly used for more severe neuropathic pain.
Tarsal tunnel syndrome is the foot’s equivalent of carpal tunnel syndrome in the wrist. The tibial nerve becomes compressed as it passes through the tarsal tunnel — a narrow space inside the ankle near the heel — causing pain, tingling, and burning on the bottom of the foot.
Pain from tarsal tunnel syndrome can radiate from the heel through the arch and into the toes. It is often described as a shooting or electric pain and is typically worse after prolonged standing or walking. People with flat feet are at higher risk because the fallen arch can compress the nerve over time.
Rest and avoiding prolonged standing help in the short term. Custom orthotics that support the arch and reduce nerve compression are a highly effective conservative treatment.
Anti-inflammatory medications and corticosteroid injections can provide significant relief. Surgery to release the tarsal tunnel and decompress the nerve is an option when conservative treatments fail after several months.
A stress fracture is a tiny crack in one of the bones of the foot, most commonly in the metatarsal bones. Unlike a full break, stress fractures develop from repetitive impact over time — common in runners, military recruits, and people who suddenly increase their activity level.
The pain typically develops gradually and worsens with activity. It is usually localized to a specific spot on the foot and is tender to touch. Unlike soft tissue injuries, stress fracture pain does not improve significantly with rest within a session — it tends to get worse the longer you continue the activity.
Stop the aggravating activity immediately. Stress fractures require rest above all else — continuing to put weight on a stress fracture can cause a complete break.
A doctor will usually confirm the diagnosis with X-rays or an MRI. Treatment involves immobilization with a boot or cast for several weeks. Returning to activity is done gradually under medical supervision to avoid re-injury.

Plantar warts are hard, grainy growths on the bottom of the foot caused by the human papillomavirus (HPV). The virus enters through small cuts or abrasions on the sole. Plantar warts most commonly develop in weight-bearing areas like the heel and ball of the foot and can make walking uncomfortable or painful.
Corns and calluses are thickened layers of skin that develop in response to repeated friction or pressure. While they are the body’s protective response, they can build up enough to create pain, particularly if they form over bony prominences.
Over-the-counter salicylic acid treatments can gradually dissolve plantar warts. A podiatrist can remove them more quickly using cryotherapy, laser treatment, or surgical excision. Modern Swift Microwave Therapy destroys the virus directly and has a lower recurrence rate than traditional methods.
Corns and calluses can be managed by soaking the foot and using a pumice stone to remove layers of dead skin. Wearing properly fitting shoes and using protective padding eliminates the friction that causes them to form in the first place.
Sesamoiditis is inflammation of the two small sesamoid bones located beneath the big toe joint on the ball of the foot. These pea-sized bones are embedded in the tendon and act like a pulley system, helping the big toe to push off with each step.
Sesamoiditis is common in runners, ballet dancers, and people who spend significant time on the balls of their feet. The pain is felt specifically under the big toe joint and worsens when flexing the toe or pushing off during walking or running.
Rest and reducing activity that loads the forefoot is essential. A metatarsal pad or a felt pad placed under the big toe joint offloads pressure from the sesamoids and can dramatically reduce pain.
Taping the big toe to limit movement allows the inflamed tendons to rest and heal. Low-heeled shoes reduce the amount of weight placed on the forefoot. If symptoms persist, a podiatrist may recommend steroid injections or, in rare cases, surgical removal of the damaged bone.
Both rheumatoid arthritis (RA) and osteoarthritis can cause pain on the bottom of the foot. Osteoarthritis involves the gradual wearing down of cartilage in the foot joints, causing stiffness, aching, and difficulty walking.
Rheumatoid arthritis is an autoimmune condition that causes inflammation in the joints throughout the body. Almost everyone with RA eventually develops symptoms in their feet and ankles — including the heel, arch, ball of the foot, and toes.
Gout, another form of arthritis caused by uric acid crystal build-up, most commonly attacks the big toe joint first and can produce intense, sudden pain on the sole near the ball of the foot.
Anti-inflammatory medications (NSAIDs like ibuprofen or naproxen) are a standard first-line treatment for arthritis flares in the foot. Shoe inserts redistribute pressure and reduce joint loading significantly.
For rheumatoid arthritis, disease-modifying drugs prescribed by a rheumatologist can slow joint damage. Physical therapy to maintain range of motion and foot strength is valuable for all types of arthritis.
Sometimes the bottom of your foot hurts simply because you have been on it too long. Standing for extended hours on hard surfaces, sudden increases in walking or running distance, and wearing unsupportive shoes all cause micro-stress to the tissues of the sole.
This type of pain is typically diffuse — spread across the bottom of the foot rather than pinpointed to one spot. It develops gradually over the course of the day and resolves with rest. There is often no single identifiable injury, just cumulative loading beyond what the foot can handle.
Cushioned, supportive footwear is the most immediate intervention. Anti-fatigue mats in work areas where you stand for long periods reduce ground reaction forces significantly.
The RICE method — Rest, Ice, Compression, and Elevation — is effective for overuse soreness. Gradually increasing your activity level rather than making sudden jumps in distance or duration helps your feet adapt without breaking down.
| Treatment Type | Best For | Notes |
|---|---|---|
| Rest and activity modification | All causes | First step for most conditions |
| Ice (20 min, 3x daily) | Inflammation, plantar fasciitis | Do not apply directly to skin |
| Stretching (calf and plantar fascia) | Plantar fasciitis, Achilles issues | Do before first steps in the morning |
| Over-the-counter NSAIDs | Inflammation, arthritis, metatarsalgia | Ibuprofen or naproxen |
| Supportive footwear | All causes | Foundation of long-term management |
| Custom orthotics | Flat feet, plantar fasciitis, tarsal tunnel | Prescribed by podiatrist |
| Metatarsal pads | Ball of foot pain, neuroma, sesamoiditis | Available OTC |
| Night splints | Plantar fasciitis | Keep fascia stretched during sleep |
| Physical therapy | Chronic conditions, post-injury | Strengthens intrinsic foot muscles |
| Corticosteroid injections | Persistent plantar fasciitis, neuroma | Given by a doctor |
| Surgery | When conservative methods fail | Last resort for most conditions |

Stretching is one of the most powerful tools for reducing bottom of foot pain, particularly for plantar fasciitis, tight calf muscles, and arch pain.
The calf stretch is the most important. Stand facing a wall, place your hands on it, step one foot back, and press the heel to the floor while keeping the leg straight. Hold for 30 seconds and repeat on both sides. Tight calves are a leading contributor to plantar fascia strain.
The plantar fascia stretch can be done before getting out of bed each morning. Sit on the edge of the bed, cross one foot over your knee, grab the toes, and gently pull them back toward your shin. Hold for 30 seconds. This pre-stretches the fascia before you load it with your first steps.
Rolling the bottom of your foot over a frozen water bottle or a tennis ball for two to three minutes massages the plantar fascia, increases circulation, and breaks up adhesions in the tissue.
Not all foot pain needs medical attention, but certain situations require prompt evaluation.
| See a Doctor If | Reason |
|---|---|
| Pain lasts more than two weeks without improvement | Could indicate a structural problem |
| Severe swelling, bruising, or inability to walk | May suggest a fracture or serious injury |
| Numbness, tingling, or burning throughout the foot | Signs of nerve damage or neuropathy |
| You have diabetes and any foot pain | Higher risk of serious complications |
| A visible lump or growth that is growing or changing | Needs evaluation to rule out serious causes |
| Pain follows an injury or fall | Possible fracture requires imaging |
Podiatrists specialize in foot and ankle conditions and are the most appropriate specialist for most bottom-of-foot pain. Orthopedic surgeons are involved when structural issues or surgery may be needed.
Footwear is one of the most powerful levers you have for both treating and preventing bottom-of-foot pain. The right shoe reduces ground forces, supports the arch, and protects the soft tissues of the sole.
Look for shoes with firm heel counters, adequate arch support, cushioned midsoles, and a wide enough toe box that your toes are not compressed. Running shoes should be replaced every 300-500 miles, as the cushioning degrades with use even if the outside still looks intact.
Avoid completely flat shoes, flip flops, and high heels for daily wear. These force the plantar fascia and metatarsals to absorb forces they are not designed to handle without support.
Custom orthotics prescribed by a podiatrist offer a superior level of support compared to off-the-shelf insoles, particularly for structural issues like flat feet, high arches, and overpronation.
Prevention is significantly easier than treatment for most conditions causing bottom-of-foot pain. A few consistent habits make a major difference over time.
Maintain a healthy body weight. Each extra pound adds roughly three to four pounds of force on the foot during walking. Reducing body weight directly reduces the load on every structure in the sole.
Stretch your calves and feet daily, especially if you run or stand for long periods. Tight calf muscles are linked to plantar fasciitis, Achilles tendinitis, and several other painful foot conditions.
Wear supportive shoes that fit correctly. Have your feet professionally measured — feet change shape with age, and wearing the wrong size is a leading preventable cause of foot pain.
Replace athletic shoes regularly. Worn-out cushioning is a major contributor to overuse injuries and stress fractures in active people.
Morning heel pain that eases after a few minutes of walking is the classic sign of plantar fasciitis. The fascia tightens during rest and is suddenly stressed with the first steps of the day.
Ball of foot pain during walking is most commonly caused by metatarsalgia, Morton’s neuroma, or sesamoiditis. Switching to wider, cushioned shoes and using metatarsal pads usually helps significantly.
Yes, absolutely. Shoes without adequate arch support, shoes that are too tight or too loose, high heels, and worn-out athletic shoes are among the leading causes of plantar fasciitis, metatarsalgia, and nerve pain.
A burning sensation on the sole is typically a nerve symptom. Common causes include peripheral neuropathy (often linked to diabetes), tarsal tunnel syndrome, Morton’s neuroma, or burning feet syndrome.
Stress fracture pain develops gradually, is localized to one specific tender spot on the foot, and worsens with continued activity rather than improving. It requires imaging (X-ray or MRI) for a proper diagnosis.
Yes. Flat feet alter how forces travel through the foot, placing extra strain on the plantar fascia, tendons, and joints. The result is often arch pain, heel pain, or aching throughout the sole after activity.
Rest, applying ice for 20 minutes three times per day, stretching the calf and plantar fascia, and switching to supportive footwear are the fastest home interventions. The RICE method (Rest, Ice, Compression, Elevation) works well for acute soreness.
With consistent treatment, most cases of plantar fasciitis improve within three to six months. Without treatment or with continued aggravation, it can become a chronic condition lasting a year or more.
Light walking that does not worsen pain is generally acceptable. High-impact activity like running or jumping should be avoided until the cause of the pain is identified and managed. If walking is severely painful, see a doctor before continuing.
See a doctor if pain has not improved after two weeks of home care, if you cannot bear weight on the foot, if you have significant swelling or bruising, if you have diabetes, or if there is numbness or tingling present.
Why does the bottom of my foot hurt is a question with many possible answers, and finding the right one is the key to getting real, lasting relief. From plantar fasciitis — the most common culprit — to Morton’s neuroma, stress fractures, neuropathy, and arthritis, the sole of your foot can be affected by a wide range of conditions.
The good news is that the majority of bottom-of-foot pain responds well to conservative treatment: the right footwear, consistent stretching, targeted rest, and anti-inflammatory measures.
Start with the location of your pain and the pattern of your symptoms to narrow down the likely cause. If home treatment does not improve things within two weeks, or if your pain is severe, a podiatrist or orthopedic specialist can provide a definitive diagnosis and a personalized treatment plan. You do not have to keep living with foot pain — most causes are very treatable with the right approach.