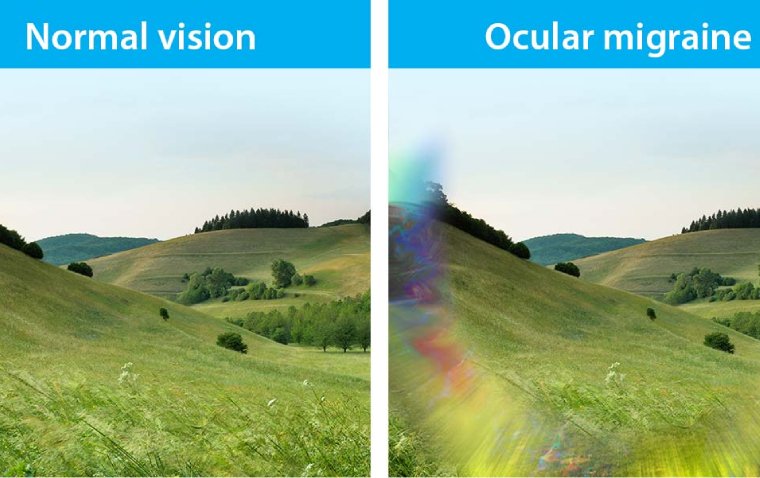
Why am I suddenly getting ocular migraines? If you have been asking yourself this lately, you are far from alone. Ocular migraines — also called retinal migraines or visual migraines — are episodes of temporary visual disturbances that can appear without warning.
They can involve flashing lights, zigzag patterns, blind spots, or even short-term vision loss in one eye.
While they are rarely dangerous, their sudden onset can be alarming and confusing. This guide breaks down every major cause, trigger, and treatment option so you know exactly what is happening and what to do next.
An ocular migraine is a type of migraine that primarily produces visual symptoms rather than — or alongside — head pain.
The American Migraine Foundation notes that “ocular migraine” is a common umbrella term used to describe migraines that cause visual disturbances, even without a headache. Medically, this covers two main conditions: migraine with aura and retinal migraine.
Despite the name, the problem does not always originate in your eyes. In most cases, it stems from the brain’s visual cortex processing signals abnormally.
These two conditions are often confused but are clinically distinct. Understanding the difference matters for your diagnosis and treatment.
| Feature | Migraine With Aura | Retinal Migraine |
|---|---|---|
| Eyes affected | Both eyes | One eye only |
| Duration | 5–60 minutes | Under 60 minutes |
| Symptoms | Zigzag lines, flashing lights, blind spots | Temporary vision loss or blindness in one eye |
| Risk level | Generally benign | Rarely, can cause permanent vision loss |
| Associated headache | Often follows aura | May or may not follow |
Migraine with aura affects both eyes because the disturbance is happening in the brain’s visual cortex. A retinal migraine affects only one eye because it involves blood vessel changes or spreading depression directly in the retina of that eye.
The sudden onset of ocular migraines is one of the most common reasons people visit neurologists and ophthalmologists. Here are the most evidence-backed causes.
The underlying brain mechanism behind most ocular migraines is called cortical spreading depression (CSD). This is a slow wave of electrical and chemical activity that moves across the brain’s visual cortex.
When this wave reaches nerve cells responsible for processing visual signals, those cells fire abnormally. The result is the characteristic visual aura — shimmering lights, zigzag lines, or expanding blind spots.
CSD can be triggered by dozens of factors, which is why ocular migraines can appear to come “out of nowhere.”
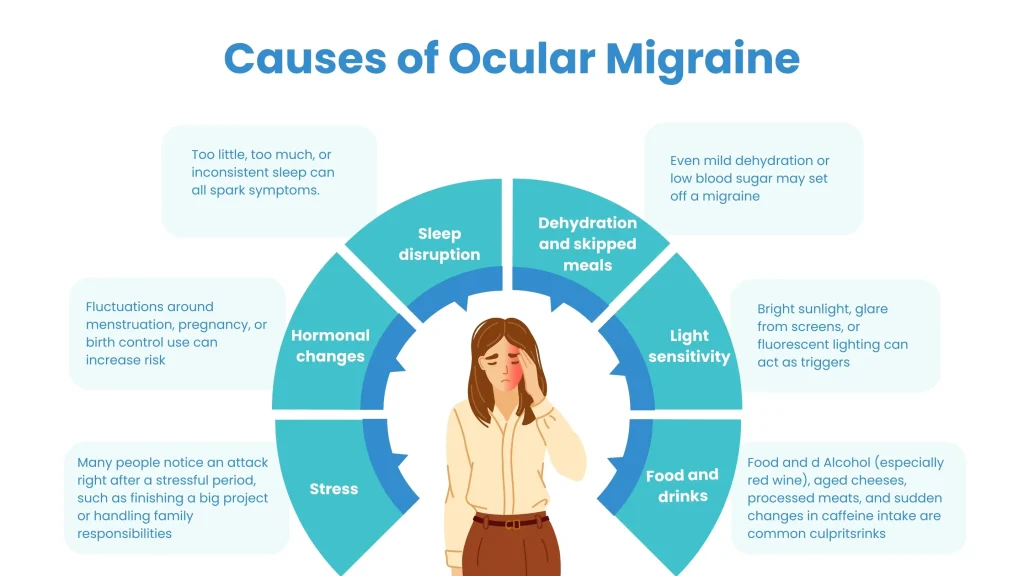
Any abrupt shift in your daily routine can trigger the first ocular migraine you have ever experienced. Your brain is highly sensitive to changes in its internal environment.
Common lifestyle disruptions include jet lag from travel, a sudden change in sleep schedule, or starting a new demanding job. Even a single night of poor sleep can lower your migraine threshold significantly.
Dr. Carolyn Bernstein of Brigham and Women’s Hospital notes that “your period may change when you hit perimenopause, or you may get a poor night’s sleep” — either of which can spark a sudden ocular migraine.
Not drinking enough water is one of the most overlooked and most common triggers for ocular migraines. The brain is extremely sensitive to fluid balance.
When you are dehydrated, blood volume drops slightly, which can reduce cerebral blood flow. This creates the right conditions for cortical spreading depression to occur.
Alcohol is a double trigger here — it both dehydrates the body and acts as a direct vasodilator, making it a frequent culprit when ocular migraines appear “suddenly.”
Hormonal shifts are among the leading reasons women suddenly start getting ocular migraines, often in their 30s and 40s. Estrogen plays a key role in regulating brain chemicals connected to pain pathways.
Drops in estrogen during menstruation, perimenopause, or menopause can trigger migraine attacks. Starting, stopping, or switching hormonal contraceptives can also destabilize estrogen levels enough to cause sudden ocular migraines.
Research published in Reviews in Obstetrics & Gynecology found that women on oral contraceptives who experience migraines with aura are four times more likely to have worsening headache symptoms.
Stress is both a trigger and a consequence of ocular migraines. When you are under emotional or physical stress, your body releases cortisol and other stress hormones.
These hormones cause blood vessels to constrict and neurons to become hyperexcitable — exactly the conditions that promote cortical spreading depression. After the migraine passes, the experience itself creates more stress, which can trigger the next episode.
If your ocular migraines started during a period of intense work pressure, a life change, or emotional upheaval, stress is likely the primary driver.
Elevated blood pressure strains the delicate blood vessels in and around the eye and brain. People are significantly more likely to experience a migraine when blood pressure is high.
A study published in Neurology found a correlation between menopausal women with migraines and high blood pressure. If you have recently been diagnosed with hypertension or have stopped taking blood pressure medication, this could explain a sudden increase in ocular migraines.
Managing blood pressure through diet, exercise, and medication can reduce migraine frequency noticeably.
Extended screen exposure is a modern trigger that has grown significantly in importance over the past decade. Staring at screens for hours causes digital eye strain, which taxes the visual processing centers of the brain.
Flickering screens, high-refresh-rate monitors, and fluorescent overhead lighting all contribute. Fluorescent lights in particular have been shown to trigger ocular migraines in susceptible individuals due to their invisible but rapid flicker.
If you recently started a new job requiring long screen hours, or switched to a different monitor setup, this could be contributing.
Caffeine has a paradoxical relationship with migraines. In small amounts, it can relieve migraine pain by constricting blood vessels. In large daily doses, it raises your baseline migraine risk.
More importantly, if you have been drinking large amounts of coffee and suddenly cut back, caffeine withdrawal can trigger intense migraines including ocular migraines. The sudden change in caffeine intake — not necessarily the caffeine itself — is often the real trigger.
When blood glucose levels drop below normal (hypoglycemia), a migraine can be triggered relatively quickly. Skipping meals or following very low-calorie diets are common causes.
The brain runs almost entirely on glucose. When supply drops, neurons become stressed and excitability increases — setting the stage for an ocular migraine episode. Eating regular, balanced meals is one of the simplest preventive strategies.
Cigarette smoke — including second-hand exposure — is a recognized migraine trigger. Nicotine causes blood vessel constriction, which can impair circulation to the retina and visual cortex.
If you or someone in your household recently started smoking, or if you have increased your exposure to smoky environments, this could be a contributing factor.
Changes in barometric pressure, excessive heat, and shifts in humidity have all been linked to migraine onset. Weather-related triggers are harder to control but important to recognize.
Some people notice they get ocular migraines more frequently during storm systems, heat waves, or when traveling to high altitudes. Altitude itself is a recognized trigger because lower oxygen levels affect cerebral blood flow.
If you have a family history of migraines, you are significantly more likely to develop them yourself. Research consistently shows a strong genetic component in migraine susceptibility.
This means you may have carried a predisposition for years without symptoms. A new trigger — stress, hormonal change, dehydration — can “unlock” that genetic vulnerability for the first time, making ocular migraines appear suddenly even in adulthood.
Bending down to pick something up, sudden heavy lifting, or intense exercise can trigger an ocular migraine in some people. This is partly because rapid changes in body position cause a sudden shift in intracranial pressure.
Exercise-induced ocular migraines are more common in those who are already susceptible and are exercising in heat or without adequate hydration.
| Trigger Category | Specific Examples | How It Triggers Ocular Migraine |
|---|---|---|
| Dehydration | Insufficient water, alcohol consumption | Reduces cerebral blood flow |
| Hormonal | Menstruation, menopause, birth control pills | Estrogen drops disrupt brain chemistry |
| Stress | Work pressure, life changes, poor sleep | Releases cortisol, constricts vessels |
| Diet | Caffeine, MSG, nitrates, tyramine-rich foods | Excites neurons, alters blood vessels |
| Environmental | Bright lights, fluorescent lights, screens | Overstimulates visual cortex |
| Physical | Bending over, exercise, high altitude | Shifts intracranial pressure |
| Medical | High blood pressure, smoking | Strains retinal and cerebral vessels |
| Genetic | Family history of migraines | Inherited low migraine threshold |
Recognizing the symptoms helps you distinguish an ocular migraine from more serious conditions like a stroke or retinal detachment.
Visual symptoms typically last between 5 and 30 minutes, rarely exceeding 60 minutes. They include:
Shimmering or scintillating lights that often start near the center of vision and expand outward. Zigzag or arc-shaped lines, sometimes called a “fortification spectrum” because they resemble the walls of a fortress. Blind spots (scotoma) or a dark patch in the center of the visual field. Temporary blurring or dimming of vision. In retinal migraines specifically, temporary complete vision loss in one eye.
A key diagnostic feature: in migraine with aura, symptoms persist even when you close your eyes, confirming the disturbance is in the brain rather than the eyes themselves.
While most ocular migraines are benign, some visual symptoms can signal a medical emergency. Seek immediate care if you experience any of the following.
Vision loss that does not resolve within one hour. Sudden vision changes in one eye accompanied by eye pain. Visual disturbances alongside numbness, weakness, facial drooping, or difficulty speaking — these can be stroke symptoms. A first-ever ocular migraine in someone over 50 with no history of migraines. Vision loss following head trauma.
These red-flag symptoms require emergency evaluation to rule out retinal artery occlusion, retinal detachment, transient ischemic attack (TIA), or stroke.
There is no single test that confirms an ocular migraine diagnosis. Your doctor will rely on your symptom history, a physical exam, and ruling out other causes.
Your healthcare provider may order an eye examination, blood pressure evaluation, neurological assessment, or imaging studies like MRI or CT scan if they suspect a non-migraine cause.
Keeping a detailed headache diary before your appointment will significantly aid your doctor. Include what you were doing, eating, drinking, your stress level, sleep quality, and the exact timing and nature of visual symptoms.
Most ocular migraine episodes resolve on their own within 30 to 60 minutes. While waiting for symptoms to pass, the following steps can help.
Stop driving or operating machinery immediately if visual disturbances begin. Rest in a quiet, dark room. Apply a cool compress to your forehead. Stay still and avoid bending over. Stay hydrated — drink water slowly.
If you experience ocular migraines frequently, your doctor may recommend preventive treatment. The following medications have evidence supporting their use.
| Medication Class | Examples | How They Help |
|---|---|---|
| Calcium channel blockers | Verapamil, Nifedipine | Reduce vascular spasm |
| Beta-blockers | Propranolol, Metoprolol | Stabilize blood vessel tone |
| Antiepileptic drugs | Topiramate, Valproate | Reduce neuronal excitability |
| Antidepressants | Amitriptyline | Modulate pain pathways |
| CGRP inhibitors | Ajovy (fremanezumab) | Block migraine-triggering peptide |
| Aspirin (low dose) | Daily low-dose aspirin | May reduce retinal migraine risk |
CGRP (calcitonin gene-related peptide) inhibitors are among the newest and most targeted preventive options. They work by blocking a peptide that plays a central role in triggering migraines and are particularly effective for frequent migraine sufferers.
Many people significantly reduce ocular migraine frequency through consistent lifestyle changes. These are often the most sustainable long-term solutions.
Hydration: Aim for at least 8–10 glasses of water per day. Increase intake during exercise, hot weather, or alcohol consumption.
Sleep consistency: Go to bed and wake up at the same time every day. Irregular sleep is one of the strongest modifiable migraine triggers.
Stress management: Regular yoga, meditation, deep breathing exercises, and moderate aerobic exercise all reduce cortisol levels and lower migraine frequency.
Diet adjustments: Identify and avoid personal food triggers. Common ones include aged cheeses, processed meats, artificial sweeteners (aspartame), MSG, red wine, and foods high in tyramine.
Screen hygiene: Follow the 20-20-20 rule — every 20 minutes, look at something 20 feet away for 20 seconds. Use blue light filters and adjust screen brightness.
Migraine diary: Tracking patterns over 4–8 weeks often reveals specific, actionable triggers you can eliminate.
A migraine diary is one of the most recommended tools by neurologists. It does not need to be complicated to be useful.
Record the date and time each episode begins and ends. Note what you ate and drank in the 24 hours before. Log sleep quality and duration. Include your stress level (1–10 scale). Note weather changes, exercise, and any medications taken.
After 4 to 8 weeks, patterns usually become visible. Many people discover their triggers are combinations — for example, poor sleep plus caffeine plus stress — rather than a single cause.
With the average adult spending more than 7 hours per day on screens, digital eye strain has become a primary modern trigger for ocular migraines. This is increasingly relevant as remote work, streaming, and smartphone use continue to grow.
Blue light from screens does not directly cause migraines, but screen glare, extended focus, reduced blinking, and flickering artificial lighting all contribute to visual fatigue that can lower the migraine threshold.
Using anti-glare screen protectors, adjusting monitor height and distance, taking regular visual breaks, and ensuring proper lighting in your workspace are all practical steps.
Women are two to three times more likely to experience migraines than men, and hormonal factors are a major reason. Ocular migraines in women frequently correlate with specific hormonal events.
Menstrual migraines occur due to the sharp drop in estrogen just before menstruation. Perimenopause and menopause bring erratic estrogen fluctuations that can cause ocular migraines to appear for the first time or worsen after years of stability. Pregnancy can either improve or worsen migraine patterns depending on the individual.
If you are a woman who has suddenly started getting ocular migraines and are in your late 30s or 40s, perimenopause-related hormonal changes deserve serious consideration. Discuss this with your gynecologist or neurologist.
One of the most common fears when experiencing ocular migraine for the first time is that it might be a stroke. Here is how to tell them apart.
| Feature | Ocular Migraine | Stroke |
|---|---|---|
| Onset | Gradual (builds over minutes) | Sudden (seconds) |
| Visual pattern | Shimmering, expanding, geometric | Abrupt loss, blurring |
| Duration | 5–60 minutes, then resolves | Does not resolve quickly |
| Other symptoms | Headache may follow | Weakness, speech difficulty, facial drooping |
| Both eyes or one | Aura: both eyes. Retinal: one eye | Often one side of vision |
If symptoms disappear within an hour with no other neurological signs, an ocular migraine is far more likely than a stroke. However, if you are unsure — especially if this is your first episode — seek emergency care. It is always better to rule out a stroke.
You should see a doctor if you have never had an ocular migraine before and suddenly develop one. Your first episode warrants evaluation to exclude serious conditions.
Also visit your doctor if episodes are increasing in frequency, if visual symptoms last longer than one hour, if you experience pain in or around the eye, or if any neurological symptoms accompany the visual disturbance.
Your doctor may refer you to a neurologist, ophthalmologist, or neuro-ophthalmologist depending on your specific symptoms and history.
Yes — stress hormones constrict blood vessels and excite neurons, which can trigger cortical spreading depression and produce visual aura symptoms independently of any other trigger.
Most ocular migraines are benign and resolve on their own. However, retinal migraines in rare cases can lead to permanent vision loss, so frequent episodes should always be evaluated by a doctor.
Yes. Even mild dehydration reduces cerebral blood flow, lowering your migraine threshold and making an episode more likely to occur, especially combined with other triggers.
No. Many people experience the visual disturbances of an ocular migraine with no headache at all. These are sometimes called “silent migraines” or “acephalgic migraines.”
Visual symptoms typically last between 5 and 30 minutes and almost always resolve within 60 minutes. If symptoms persist beyond one hour, seek medical attention immediately.
Yes. Extended screen use causes visual fatigue and overstimulates the visual cortex, which can lower the threshold for an ocular migraine, especially under poor lighting conditions.
Yes. Contraceptives containing estrogen can trigger ocular migraines in susceptible women. Women who experience migraines with aura are generally advised to avoid estrogen-containing contraceptives.
Common dietary triggers include aged cheeses, red wine, processed meats, MSG, artificial sweeteners like aspartame, and foods high in tyramine. Triggers are individual, so keeping a food diary helps identify yours.
Yes. Elevated blood pressure strains retinal and cerebral blood vessels, which can precipitate an ocular migraine. If you have uncontrolled hypertension, it may be contributing to your episodes.
There is no cure, but most people can significantly reduce frequency and severity through trigger avoidance, lifestyle changes, and, when necessary, preventive medications prescribed by a doctor.
Why am I suddenly getting ocular migraines? The answer is rarely a single cause. Ocular migraines emerge from a combination of genetic predisposition, lifestyle triggers, hormonal shifts, and neurological sensitivity.
Whether it is a new source of stress, a hormonal change in your 40s, chronic dehydration, or increasing screen time — each factor lowers your migraine threshold until one episode breaks through.
The good news is that most ocular migraines are manageable. With careful trigger tracking, hydration, sleep consistency, stress reduction, and medical guidance when needed, most people reduce both frequency and severity significantly.
Always take a first-ever episode seriously and see a doctor to rule out more serious causes. Once you understand your personal triggers, you have the tools to take real control over your ocular migraine patterns in 2026 and beyond.